Overview and Anatomy
In many
cases, MRI results lead to changes in the proposed management. One study
determined that about one third of all diagnostic arthroscopies need
not be performed if MRI is used; another study showed that the use of
MRI prevented 51% of diagnostic arthroscopic procedures; and a third
study showed that with the use of MRI, the morbidity associated with
arthroscopy was avoided.[15]
MRIs show many of the essential characteristics of meniscal tears critical to management, such as their location, shape, length, and depth. In this way, MRI helps to make an accurate assessment of stability and of the likelihood of tear propagation, and it enables one to determine whether the meniscal tear can be repaired. It is advantageous to know ahead of time if a given meniscal tear can be repaired, because the additional equipment, surgical assistants, and time needed for repair can be anticipated. Patients also benefit from knowing early on whether surgery is necessary. The recovery time for meniscal repair is longer than that for partial meniscectomy (PM). Patients may want to time surgery to fit with their other obligations.[1, 15, 17, 18]
When combined with clinical data, such as the patient's age, athletic requirements, and physical findings (eg, possible associated ligamentous injuries), a treatment plan may be developed by assessing the need for and timing of surgery and by determining the type of surgery (meniscal debridement, rasping, repair, partial or total resection, or meniscal transplantation). MRI may be used to identify other injuries, such as ligament tears, especially anterior cruciate ligament (ACL) tears, the presence of which may also influence the decision whether to perform surgery.[1, 15, 17]
With MRI, physicians may obtain images in several planes, providing multiple perspectives on meniscal and ligamentous injuries. Other advantages include the following:
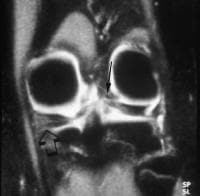
Centrally, the normal meniscus is composed of 2 separate triangular structures: the anterior horn and the posterior horn. The apices (free edges or inner margins) appear as sharp points of the triangle facing each other (see the first image below). On the lateral side of the knee, the triangular anterior and posterior horns of the LM are equal in size (see the second image below). On the medial side of the knee, the posterior horn of the MM is larger than the anterior horn (see the third image below).[13]
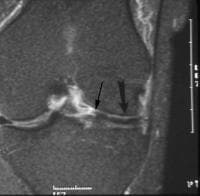
 Coronal
fat-saturated proton density–weighted image shows abnormal signal
intensity in the posterior horn of the medial meniscus (MM) extending to
the undersurface near the junction with the joint capsule. Such tears
may be missed on arthroscopy because that part of the knee joint is
difficult to access. Also present is a tear to the posterior medial horn
of the lateral meniscus (LM) as it slopes obliquely inward. A
false-positive diagnosis of meniscal tear can be made when one evaluates
this region because of the magic angle effect. Tears persist when the
echo time (TE) is varied and when T2-weighted images are obtained. True
tears can also be confirmed by visualizing them on sagittal or axial
projections.
Coronal
fat-saturated proton density–weighted image shows abnormal signal
intensity in the posterior horn of the medial meniscus (MM) extending to
the undersurface near the junction with the joint capsule. Such tears
may be missed on arthroscopy because that part of the knee joint is
difficult to access. Also present is a tear to the posterior medial horn
of the lateral meniscus (LM) as it slopes obliquely inward. A
false-positive diagnosis of meniscal tear can be made when one evaluates
this region because of the magic angle effect. Tears persist when the
echo time (TE) is varied and when T2-weighted images are obtained. True
tears can also be confirmed by visualizing them on sagittal or axial
projections.  Sagittal
fat-saturated proton density–weighted image of the lateral compartment
shows the relative equal size of the anterior and posterior horns of the
lateral meniscus. The meniscal body has the normal configuration of a
bow tie.
Sagittal
fat-saturated proton density–weighted image of the lateral compartment
shows the relative equal size of the anterior and posterior horns of the
lateral meniscus. The meniscal body has the normal configuration of a
bow tie.  Sagittal
fat-saturated proton density–weighted image of the medial compartment
shows the larger posterior horn (arrowhead) and the smaller anterior
horn. Peripherally (medially for the medial meniscus [MM] and
laterally for the lateral meniscus [LM]), the menisci have a bow-tie
configuration, as shown in the images below. The anterior and posterior
horns are taller than the thinner and interposed body of the meniscus.
Sagittal
fat-saturated proton density–weighted image of the medial compartment
shows the larger posterior horn (arrowhead) and the smaller anterior
horn. Peripherally (medially for the medial meniscus [MM] and
laterally for the lateral meniscus [LM]), the menisci have a bow-tie
configuration, as shown in the images below. The anterior and posterior
horns are taller than the thinner and interposed body of the meniscus.
 Sagittal
fat-saturated proton density–weighted image demonstrates the concave
superior meniscal surface (arrows), which improves contact with the
femoral epicondyles, and a flat undersurface, which improves contact
with the tibial plateau. The periphery (outer edges) is thicker than the
central portion (arrowhead), allowing for firm attachment to the joint
capsule. Note the normal bow-tie appearance of the meniscal body.
Sagittal
fat-saturated proton density–weighted image demonstrates the concave
superior meniscal surface (arrows), which improves contact with the
femoral epicondyles, and a flat undersurface, which improves contact
with the tibial plateau. The periphery (outer edges) is thicker than the
central portion (arrowhead), allowing for firm attachment to the joint
capsule. Note the normal bow-tie appearance of the meniscal body. 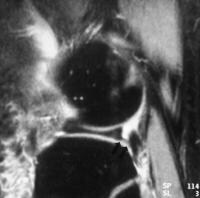 Sagittal
fat-saturated proton density–weighted image shows the inferior
fascicle. In this location, the superior fascicle is not present. Note
the normal bow-tie appearance of the meniscal body.
Sagittal
fat-saturated proton density–weighted image shows the inferior
fascicle. In this location, the superior fascicle is not present. Note
the normal bow-tie appearance of the meniscal body.  Coronal
proton density–weighted image shows extensive grade 2 signal intensity
in the anterior and posterior horns of the medial meniscus. However, the
signal intensity does not extend to a joint surface. Both
menisci have anterior and posterior roots, which attach the anterior and
posterior horns to the tibial plateau, on either side of the centrally
placed tibial spine (see the image below). These attachments are
referred to as roots.[13, 20]
Coronal
proton density–weighted image shows extensive grade 2 signal intensity
in the anterior and posterior horns of the medial meniscus. However, the
signal intensity does not extend to a joint surface. Both
menisci have anterior and posterior roots, which attach the anterior and
posterior horns to the tibial plateau, on either side of the centrally
placed tibial spine (see the image below). These attachments are
referred to as roots.[13, 20]
 Sagittal proton density–weighted image shows the tibial insertion site of the posterior horn of the medial meniscus (MM). Popliteus tendon and sheath
Sagittal proton density–weighted image shows the tibial insertion site of the posterior horn of the medial meniscus (MM). Popliteus tendon and sheath
The popliteus tendon and its accompanying sheath course through the posterolateral portion of the posterior horn of the LM in an oblique anterosuperior to posteroinferior direction. It is seen on the more lateral images of the LM (see the images below).
 Coronal
proton density–weighted image shows the ligament of Wrisberg
originating from the posterior medial horn of the medial meniscus and
passing obliquely upwards (arrow) to attach to the posterolateral aspect
of the medial femoral epicondyle.
Coronal
proton density–weighted image shows the ligament of Wrisberg
originating from the posterior medial horn of the medial meniscus and
passing obliquely upwards (arrow) to attach to the posterolateral aspect
of the medial femoral epicondyle. 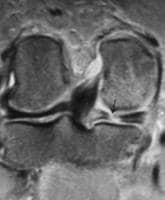 Coronal
fat-saturated proton density–weighted image shows the popliteus tendon
originating from an undulation of the lateral femoral condyle. From
there, it passes through the popliteus recess to insert on the proximal
posterior tibial metaphysis. A radial tear (arrow) is present in the
posterior horn of the medial meniscus. Two fascicles connect
the posterior horn of the LM at the popliteus tendon sheath level to the
joint capsule. The inferior fascicle is seen on the more lateral images
through the tendon. Here, the superior fascicle is absent. More
medially, both superior and inferior fascicles are present. The most
medical images through the tendon show the superior fascicle and absence
of the inferior fascicle. The thickness of the popliteus tendon sheath
varies in size from a thin line to a thick band.
Coronal
fat-saturated proton density–weighted image shows the popliteus tendon
originating from an undulation of the lateral femoral condyle. From
there, it passes through the popliteus recess to insert on the proximal
posterior tibial metaphysis. A radial tear (arrow) is present in the
posterior horn of the medial meniscus. Two fascicles connect
the posterior horn of the LM at the popliteus tendon sheath level to the
joint capsule. The inferior fascicle is seen on the more lateral images
through the tendon. Here, the superior fascicle is absent. More
medially, both superior and inferior fascicles are present. The most
medical images through the tendon show the superior fascicle and absence
of the inferior fascicle. The thickness of the popliteus tendon sheath
varies in size from a thin line to a thick band.
Structures in the coronal plane
This is the best plane in which to image the meniscal bodies (see the images below). Each meniscal body looks like a triangle with the pointed apex in the innermost part of the meniscus. The anterior and posterior horns appear as flat slabs. The root of the posterior horn of the LM is directed obliquely upward from a lateral to medial direction. The popliteus recess is located in the outer portion of the lateral joint compartment. It can be identified either by the presence of joint fluid within it or by the popliteus tendon originating from the distal lateral femur, above the joint, and passing through the sheath to insert on the back of the proximal tibia.[13, 21]
 Coronal
fat-saturated proton density–weighted image of the mid knee shows the
normal appearance of the body of the medial and lateral menisci. The
apices (inner portions) are the thinnest part of the meniscus and are
more central in the knee joint. The periphery, meniscal bases, outer
portion (arrow and arrowhead) is the thickest part and contains the
blood vessels supplying the meniscus.
Coronal
fat-saturated proton density–weighted image of the mid knee shows the
normal appearance of the body of the medial and lateral menisci. The
apices (inner portions) are the thinnest part of the meniscus and are
more central in the knee joint. The periphery, meniscal bases, outer
portion (arrow and arrowhead) is the thickest part and contains the
blood vessels supplying the meniscus.  Coronal
fat-saturated proton density–weighted image shows the relative size of
the posterior horns of the medial and lateral menisci. The posterior
horn of the medial meniscus (left arrow) is thicker than the posterior
horn of the lateral meniscus (right arrow). Note the normal dark
appearance (relative lack of signal intensity) in the menisci. The
medial portion of the posterior horn of the lateral meniscus (ie, the
meniscus on top of the fibula) is directed upward obliquely, from a
lateral to medial direction. This is its normal course.
Coronal
fat-saturated proton density–weighted image shows the relative size of
the posterior horns of the medial and lateral menisci. The posterior
horn of the medial meniscus (left arrow) is thicker than the posterior
horn of the lateral meniscus (right arrow). Note the normal dark
appearance (relative lack of signal intensity) in the menisci. The
medial portion of the posterior horn of the lateral meniscus (ie, the
meniscus on top of the fibula) is directed upward obliquely, from a
lateral to medial direction. This is its normal course.  Coronal
fat-saturated proton density–weighted image shows the popliteus recess
containing joint fluid and located between the lateral aspect of the
posterior horn of the lateral meniscus and the joint capsule. An
extensive tear is present in the posterior horn of the medial meniscus
(arrow). Note the normal oblique upward orientation of the posterior
medial horn of the lateral meniscus.
Coronal
fat-saturated proton density–weighted image shows the popliteus recess
containing joint fluid and located between the lateral aspect of the
posterior horn of the lateral meniscus and the joint capsule. An
extensive tear is present in the posterior horn of the medial meniscus
(arrow). Note the normal oblique upward orientation of the posterior
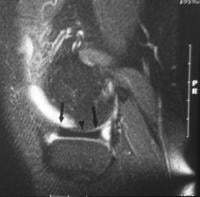
medial horn of the lateral meniscus.  Coronal
fat-saturated proton density–weighted image shows the dark appearing
popliteus tendon (arrows) passing through the popliteus recess. The
posterior medial horn of the lateral meniscus is directed obliquely
upward. Coronal
fat-saturated proton density–weighted image shows abnormal signal
intensity in the posterior horn of the medial meniscus (MM) extending to
the undersurface near the junction with the joint capsule. Such tears
may be missed on arthroscopy because that part of the knee joint is
difficult to access. Also present is a tear to the posterior medial horn
of the lateral meniscus (LM) as it slopes obliquely inward. A
false-positive diagnosis of meniscal tear can be made when one evaluates
this region because of the magic angle effect. Tears persist when the
echo time (TE) is varied and when T2-weighted images are obtained. True
tears can also be confirmed by visualizing them on sagittal or axial
projections.
Coronal
fat-saturated proton density–weighted image shows the dark appearing
popliteus tendon (arrows) passing through the popliteus recess. The
posterior medial horn of the lateral meniscus is directed obliquely
upward. Coronal
fat-saturated proton density–weighted image shows abnormal signal
intensity in the posterior horn of the medial meniscus (MM) extending to
the undersurface near the junction with the joint capsule. Such tears
may be missed on arthroscopy because that part of the knee joint is
difficult to access. Also present is a tear to the posterior medial horn
of the lateral meniscus (LM) as it slopes obliquely inward. A
false-positive diagnosis of meniscal tear can be made when one evaluates
this region because of the magic angle effect. Tears persist when the
echo time (TE) is varied and when T2-weighted images are obtained. True
tears can also be confirmed by visualizing them on sagittal or axial
projections.  Coronal
fat-saturated proton density–weighted image of the posterior portion of
the knee joint. A circular, fluid-filled structure (arrow) is present
in the upper portion of the most medial portion of the posterior horn of
the medial meniscus; it represents a meniscal cyst. The
insertion of the semimembranosus tendon is located posterior along the
subarticular surface of the medial aspect of the proximal tibial
metaphysis (see the images below). This is not to be confused with a
displaced meniscal fragment.
Coronal
fat-saturated proton density–weighted image of the posterior portion of
the knee joint. A circular, fluid-filled structure (arrow) is present
in the upper portion of the most medial portion of the posterior horn of
the medial meniscus; it represents a meniscal cyst. The
insertion of the semimembranosus tendon is located posterior along the
subarticular surface of the medial aspect of the proximal tibial
metaphysis (see the images below). This is not to be confused with a
displaced meniscal fragment.
 Sagittal
fat-saturated proton density–weighted image of the posterior knee
compartment shows the normal insertion (arrow) of the semimembranosus
tendon. The insertion site is near the posterior horn of the medial
meniscus (MM), and it is not to be mistaken for a displaced meniscal
fragment.
Sagittal
fat-saturated proton density–weighted image of the posterior knee
compartment shows the normal insertion (arrow) of the semimembranosus
tendon. The insertion site is near the posterior horn of the medial
meniscus (MM), and it is not to be mistaken for a displaced meniscal
fragment.  Sagittal
fat-saturated proton density–weighted image of the paramedian portion
of the lateral joint compartment. The transverse intermeniscal ligament
(arrowhead) is about to unite with the anterior horn of the medial
meniscus (MM, arrow). Fat is normally present in this region and can
mimic a ligament or meniscal tear. By carefully following the course of
the ligament on sequential images and by observing a uniformly
well-defined, hypointense structure on every image, this pitfall can be
avoided. A small, ill-defined, linear soft tissue density is present
under the anterior horn. It is separated from the anterior horn by
bright fluid. This is a rare tear in this region. The brightness is
joint fluid in the tear. Meniscal flounce
Sagittal
fat-saturated proton density–weighted image of the paramedian portion
of the lateral joint compartment. The transverse intermeniscal ligament
(arrowhead) is about to unite with the anterior horn of the medial
meniscus (MM, arrow). Fat is normally present in this region and can
mimic a ligament or meniscal tear. By carefully following the course of
the ligament on sequential images and by observing a uniformly
well-defined, hypointense structure on every image, this pitfall can be
avoided. A small, ill-defined, linear soft tissue density is present
under the anterior horn. It is separated from the anterior horn by
bright fluid. This is a rare tear in this region. The brightness is
joint fluid in the tear. Meniscal flounce
A meniscal flounce is an uncommon meniscal variant characterized by a single symmetrical fold along the free edge of the meniscus. It appears as an S -shaped fold along the free edge on sagittal images and is associated with a truncated but normal meniscus on coronal images.
Normal meniscal signal intensity
The normal meniscus shows uniform, low signal intensity on T1- and T2-weighted images obtained with both conventional and fast-spin echo (FSE) sequences. The low signal is related to a lack of mobile protons in the meniscal fibrocartilage. Subsequent dephasing of hydrogen nuclei results in T2 shortening, contributing to the low signal intensity on all pulse sequences.
Fascicles of the posterior horn of the LM are best evaluated on T2-weighted sagittal images. This is due to the bright fluid in the popliteus tendon sheath and joint space contrasting with the low signal intensity of the fascicles.[22]
Discoid meniscus
Differentiation between a true discoid meniscus (DM) and a slightly larger but normal meniscus may be difficult.
On sagittal images, the DM has a thickened, bow-tie appearance on 3 consecutive sagittal images. The anterior and posterior horns of the normal meniscus are seen on several images near the intercondylar notch. With a complete DM, no distinct anterior or posterior horn is present. The normal meniscus rapidly tapers from the outer periphery to the center. The presence of equal or nearly equal meniscal height on 2 adjacent peripheral 5-mm-thick images indicates a DM. The anterior and posterior horns of the LM are normally equal in height. An asymmetric discoid LM may have an abnormally large anterior or posterior horn.[23]
On coronal views, the abnormal meniscal body extends more medially toward the intercondylar notch (see the image below).
 Coronal
fat-saturated proton density–weighted image shows irregularity to the
upper (femoral) surface of the body of the lateral meniscus (LM, outer
arrow), indicating fraying. Fraying usually occurs at the meniscal apex.
Soft tissue densities (inner arrow) are present under the apex of the
meniscus, indicating debris or a free meniscal fragment at this level.
The body of the LM is unusually thick and longer than usual, indicating a
discoid meniscus. The normal-sized medial meniscal body is present for
comparison. Discoid menisci occur about 5 times more often here than in
the LM, and they are more prone to injury. The posteromedial
horn of the MM and the anterior horn of the MM near the roots may have a
normal speckled appearance (see the images below).
Coronal
fat-saturated proton density–weighted image shows irregularity to the
upper (femoral) surface of the body of the lateral meniscus (LM, outer
arrow), indicating fraying. Fraying usually occurs at the meniscal apex.
Soft tissue densities (inner arrow) are present under the apex of the
meniscus, indicating debris or a free meniscal fragment at this level.
The body of the LM is unusually thick and longer than usual, indicating a
discoid meniscus. The normal-sized medial meniscal body is present for
comparison. Discoid menisci occur about 5 times more often here than in
the LM, and they are more prone to injury. The posteromedial
horn of the MM and the anterior horn of the MM near the roots may have a
normal speckled appearance (see the images below).
 Sagittal
fat-saturated proton density–weighted image of the paramedian portion
of the medial knee. The transverse intermeniscal ligament is about to
insert on the anterior horn of the medial meniscus (MM). The anterior
horn is normally speckled. The anterior horn is partially displaced off
the anterior surface of the tibia by a radial tear more laterally
(picture is not shown). A tear involves the posterior horn of the MM
(arrow).
Sagittal
fat-saturated proton density–weighted image of the paramedian portion
of the medial knee. The transverse intermeniscal ligament is about to
insert on the anterior horn of the medial meniscus (MM). The anterior
horn is normally speckled. The anterior horn is partially displaced off
the anterior surface of the tibia by a radial tear more laterally
(picture is not shown). A tear involves the posterior horn of the MM
(arrow). 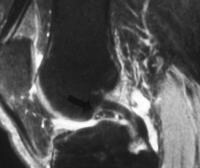 Sagittal
fat-saturated proton density-weighted image shows a well-defined, soft
tissue density in front of the posterior cruciate ligament (PCL). It is
speckled and looks like the normal posterior medial horn of the medial
meniscus (MM), but it is in the wrong place. This finding represents a
displaced meniscal tear involving the posterior medial horn. The
position of the meniscus is referred to as a double PCL because it looks
like 2 of these ligaments are present. Coronal images show
the smallest width of the meniscal body, making this plane the most
sensitive for showing meniscal enlargement. An asymmetric DM with an
enlarged body may have a wide meniscal body on coronal images but normal
anterior and posterior horns on sagittal images, emphasizing the need
for coronal images. Incomplete DM may not extend into the intercondylar
notch.
Sagittal
fat-saturated proton density-weighted image shows a well-defined, soft
tissue density in front of the posterior cruciate ligament (PCL). It is
speckled and looks like the normal posterior medial horn of the medial
meniscus (MM), but it is in the wrong place. This finding represents a
displaced meniscal tear involving the posterior medial horn. The
position of the meniscus is referred to as a double PCL because it looks
like 2 of these ligaments are present. Coronal images show
the smallest width of the meniscal body, making this plane the most
sensitive for showing meniscal enlargement. An asymmetric DM with an
enlarged body may have a wide meniscal body on coronal images but normal
anterior and posterior horns on sagittal images, emphasizing the need
for coronal images. Incomplete DM may not extend into the intercondylar
notch.
In children, grade 2 signal is frequently seen within the posterior meniscal horns. This is thought to represent normal vasculature, seen in the meniscus of a child. This disappears in adulthood.
Regarding the meniscofemoral ligaments, either the anterior or posterior ligament is present on 33% of MRIs. Both ligaments are present on 3% of examinations. One of the 2 ligaments predominates. The ligament of Humphry is best seen on sagittal images. It is occasionally seen on coronal images. The ligament of Wrisberg is best seen on posterior coronal images.[23, 24]
Meniscal degeneration
Local increases in the degree of freedom of trapped water molecules within the substance of the meniscus occurs with age, resulting in increased T2 times. The appearance is that of increased signal intensity within the substance of the meniscus on short-TE images.[22]
MRIs show many of the essential characteristics of meniscal tears critical to management, such as their location, shape, length, and depth. In this way, MRI helps to make an accurate assessment of stability and of the likelihood of tear propagation, and it enables one to determine whether the meniscal tear can be repaired. It is advantageous to know ahead of time if a given meniscal tear can be repaired, because the additional equipment, surgical assistants, and time needed for repair can be anticipated. Patients also benefit from knowing early on whether surgery is necessary. The recovery time for meniscal repair is longer than that for partial meniscectomy (PM). Patients may want to time surgery to fit with their other obligations.[1, 15, 17, 18]
When combined with clinical data, such as the patient's age, athletic requirements, and physical findings (eg, possible associated ligamentous injuries), a treatment plan may be developed by assessing the need for and timing of surgery and by determining the type of surgery (meniscal debridement, rasping, repair, partial or total resection, or meniscal transplantation). MRI may be used to identify other injuries, such as ligament tears, especially anterior cruciate ligament (ACL) tears, the presence of which may also influence the decision whether to perform surgery.[1, 15, 17]
With MRI, physicians may obtain images in several planes, providing multiple perspectives on meniscal and ligamentous injuries. Other advantages include the following:
- MRI does not expose the patient to ionizing radiation
- MRI does not normally involve the intravenous administration of contrast material, the use of which is associated with a small but definite number of adverse effects
- MRI does not require joint manipulation
- MRI is painless and can be performed in less than 35 minutes
- MRI does not require the intra-articular injection of iodinated radiographic contrast material, which is needed for arthrography
Normal Anatomy on MRIs
Structures in the sagittal planeCentrally, the normal meniscus is composed of 2 separate triangular structures: the anterior horn and the posterior horn. The apices (free edges or inner margins) appear as sharp points of the triangle facing each other (see the first image below). On the lateral side of the knee, the triangular anterior and posterior horns of the LM are equal in size (see the second image below). On the medial side of the knee, the posterior horn of the MM is larger than the anterior horn (see the third image below).[13]
Coronal
fat-saturated proton density–weighted image shows abnormal signal
intensity in the posterior horn of the medial meniscus (MM) extending to
the undersurface near the junction with the joint capsule. Such tears
may be missed on arthroscopy because that part of the knee joint is
difficult to access. Also present is a tear to the posterior medial horn
of the lateral meniscus (LM) as it slopes obliquely inward. A
false-positive diagnosis of meniscal tear can be made when one evaluates
this region because of the magic angle effect. Tears persist when the
echo time (TE) is varied and when T2-weighted images are obtained. True
tears can also be confirmed by visualizing them on sagittal or axial
projections. Sagittal
fat-saturated proton density–weighted image of the lateral compartment
shows the relative equal size of the anterior and posterior horns of the
lateral meniscus. The meniscal body has the normal configuration of a
bow tie. Sagittal
fat-saturated proton density–weighted image of the medial compartment
shows the larger posterior horn (arrowhead) and the smaller anterior
horn. Peripherally (medially for the medial meniscus [MM] and
laterally for the lateral meniscus [LM]), the menisci have a bow-tie
configuration, as shown in the images below. The anterior and posterior
horns are taller than the thinner and interposed body of the meniscus.Sagittal
fat-saturated proton density–weighted image demonstrates the concave
superior meniscal surface (arrows), which improves contact with the
femoral epicondyles, and a flat undersurface, which improves contact
with the tibial plateau. The periphery (outer edges) is thicker than the
central portion (arrowhead), allowing for firm attachment to the joint
capsule. Note the normal bow-tie appearance of the meniscal body. Sagittal
fat-saturated proton density–weighted image shows the inferior
fascicle. In this location, the superior fascicle is not present. Note
the normal bow-tie appearance of the meniscal body. Coronal
proton density–weighted image shows extensive grade 2 signal intensity
in the anterior and posterior horns of the medial meniscus. However, the
signal intensity does not extend to a joint surface. Both
menisci have anterior and posterior roots, which attach the anterior and
posterior horns to the tibial plateau, on either side of the centrally
placed tibial spine (see the image below). These attachments are
referred to as roots.[13, 20] Sagittal proton density–weighted image shows the tibial insertion site of the posterior horn of the medial meniscus (MM). Popliteus tendon and sheathThe popliteus tendon and its accompanying sheath course through the posterolateral portion of the posterior horn of the LM in an oblique anterosuperior to posteroinferior direction. It is seen on the more lateral images of the LM (see the images below).
Coronal
proton density–weighted image shows the ligament of Wrisberg
originating from the posterior medial horn of the medial meniscus and
passing obliquely upwards (arrow) to attach to the posterolateral aspect
of the medial femoral epicondyle. Coronal
fat-saturated proton density–weighted image shows the popliteus tendon
originating from an undulation of the lateral femoral condyle. From
there, it passes through the popliteus recess to insert on the proximal
posterior tibial metaphysis. A radial tear (arrow) is present in the
posterior horn of the medial meniscus. Two fascicles connect
the posterior horn of the LM at the popliteus tendon sheath level to the
joint capsule. The inferior fascicle is seen on the more lateral images
through the tendon. Here, the superior fascicle is absent. More
medially, both superior and inferior fascicles are present. The most
medical images through the tendon show the superior fascicle and absence
of the inferior fascicle. The thickness of the popliteus tendon sheath
varies in size from a thin line to a thick band. Structures in the coronal plane
This is the best plane in which to image the meniscal bodies (see the images below). Each meniscal body looks like a triangle with the pointed apex in the innermost part of the meniscus. The anterior and posterior horns appear as flat slabs. The root of the posterior horn of the LM is directed obliquely upward from a lateral to medial direction. The popliteus recess is located in the outer portion of the lateral joint compartment. It can be identified either by the presence of joint fluid within it or by the popliteus tendon originating from the distal lateral femur, above the joint, and passing through the sheath to insert on the back of the proximal tibia.[13, 21]
Coronal
fat-saturated proton density–weighted image of the mid knee shows the
normal appearance of the body of the medial and lateral menisci. The
apices (inner portions) are the thinnest part of the meniscus and are
more central in the knee joint. The periphery, meniscal bases, outer
portion (arrow and arrowhead) is the thickest part and contains the
blood vessels supplying the meniscus. Coronal
fat-saturated proton density–weighted image shows the relative size of
the posterior horns of the medial and lateral menisci. The posterior
horn of the medial meniscus (left arrow) is thicker than the posterior
horn of the lateral meniscus (right arrow). Note the normal dark
appearance (relative lack of signal intensity) in the menisci. The
medial portion of the posterior horn of the lateral meniscus (ie, the
meniscus on top of the fibula) is directed upward obliquely, from a
lateral to medial direction. This is its normal course. Coronal
fat-saturated proton density–weighted image shows the popliteus recess
containing joint fluid and located between the lateral aspect of the
posterior horn of the lateral meniscus and the joint capsule. An
extensive tear is present in the posterior horn of the medial meniscus
(arrow). Note the normal oblique upward orientation of the posterior
medial horn of the lateral meniscus. Coronal
fat-saturated proton density–weighted image shows the dark appearing
popliteus tendon (arrows) passing through the popliteus recess. The
posterior medial horn of the lateral meniscus is directed obliquely
upward. Coronal
fat-saturated proton density–weighted image shows abnormal signal
intensity in the posterior horn of the medial meniscus (MM) extending to
the undersurface near the junction with the joint capsule. Such tears
may be missed on arthroscopy because that part of the knee joint is
difficult to access. Also present is a tear to the posterior medial horn
of the lateral meniscus (LM) as it slopes obliquely inward. A
false-positive diagnosis of meniscal tear can be made when one evaluates
this region because of the magic angle effect. Tears persist when the
echo time (TE) is varied and when T2-weighted images are obtained. True
tears can also be confirmed by visualizing them on sagittal or axial
projections. Coronal
fat-saturated proton density–weighted image of the posterior portion of
the knee joint. A circular, fluid-filled structure (arrow) is present
in the upper portion of the most medial portion of the posterior horn of
the medial meniscus; it represents a meniscal cyst. The
insertion of the semimembranosus tendon is located posterior along the
subarticular surface of the medial aspect of the proximal tibial
metaphysis (see the images below). This is not to be confused with a
displaced meniscal fragment.Sagittal
fat-saturated proton density–weighted image of the posterior knee
compartment shows the normal insertion (arrow) of the semimembranosus
tendon. The insertion site is near the posterior horn of the medial
meniscus (MM), and it is not to be mistaken for a displaced meniscal
fragment. Sagittal
fat-saturated proton density–weighted image of the paramedian portion
of the lateral joint compartment. The transverse intermeniscal ligament
(arrowhead) is about to unite with the anterior horn of the medial
meniscus (MM, arrow). Fat is normally present in this region and can
mimic a ligament or meniscal tear. By carefully following the course of
the ligament on sequential images and by observing a uniformly
well-defined, hypointense structure on every image, this pitfall can be
avoided. A small, ill-defined, linear soft tissue density is present
under the anterior horn. It is separated from the anterior horn by
bright fluid. This is a rare tear in this region. The brightness is
joint fluid in the tear. Meniscal flounceA meniscal flounce is an uncommon meniscal variant characterized by a single symmetrical fold along the free edge of the meniscus. It appears as an S -shaped fold along the free edge on sagittal images and is associated with a truncated but normal meniscus on coronal images.
Normal meniscal signal intensity
The normal meniscus shows uniform, low signal intensity on T1- and T2-weighted images obtained with both conventional and fast-spin echo (FSE) sequences. The low signal is related to a lack of mobile protons in the meniscal fibrocartilage. Subsequent dephasing of hydrogen nuclei results in T2 shortening, contributing to the low signal intensity on all pulse sequences.
Fascicles of the posterior horn of the LM are best evaluated on T2-weighted sagittal images. This is due to the bright fluid in the popliteus tendon sheath and joint space contrasting with the low signal intensity of the fascicles.[22]
Discoid meniscus
Differentiation between a true discoid meniscus (DM) and a slightly larger but normal meniscus may be difficult.
On sagittal images, the DM has a thickened, bow-tie appearance on 3 consecutive sagittal images. The anterior and posterior horns of the normal meniscus are seen on several images near the intercondylar notch. With a complete DM, no distinct anterior or posterior horn is present. The normal meniscus rapidly tapers from the outer periphery to the center. The presence of equal or nearly equal meniscal height on 2 adjacent peripheral 5-mm-thick images indicates a DM. The anterior and posterior horns of the LM are normally equal in height. An asymmetric discoid LM may have an abnormally large anterior or posterior horn.[23]
On coronal views, the abnormal meniscal body extends more medially toward the intercondylar notch (see the image below).
Coronal
fat-saturated proton density–weighted image shows irregularity to the
upper (femoral) surface of the body of the lateral meniscus (LM, outer
arrow), indicating fraying. Fraying usually occurs at the meniscal apex.
Soft tissue densities (inner arrow) are present under the apex of the
meniscus, indicating debris or a free meniscal fragment at this level.
The body of the LM is unusually thick and longer than usual, indicating a
discoid meniscus. The normal-sized medial meniscal body is present for
comparison. Discoid menisci occur about 5 times more often here than in
the LM, and they are more prone to injury. The posteromedial
horn of the MM and the anterior horn of the MM near the roots may have a
normal speckled appearance (see the images below).Sagittal
fat-saturated proton density–weighted image of the paramedian portion
of the medial knee. The transverse intermeniscal ligament is about to
insert on the anterior horn of the medial meniscus (MM). The anterior
horn is normally speckled. The anterior horn is partially displaced off
the anterior surface of the tibia by a radial tear more laterally
(picture is not shown). A tear involves the posterior horn of the MM
(arrow). Sagittal
fat-saturated proton density-weighted image shows a well-defined, soft
tissue density in front of the posterior cruciate ligament (PCL). It is
speckled and looks like the normal posterior medial horn of the medial
meniscus (MM), but it is in the wrong place. This finding represents a
displaced meniscal tear involving the posterior medial horn. The
position of the meniscus is referred to as a double PCL because it looks
like 2 of these ligaments are present. Coronal images show
the smallest width of the meniscal body, making this plane the most
sensitive for showing meniscal enlargement. An asymmetric DM with an
enlarged body may have a wide meniscal body on coronal images but normal
anterior and posterior horns on sagittal images, emphasizing the need
for coronal images. Incomplete DM may not extend into the intercondylar
notch. In children, grade 2 signal is frequently seen within the posterior meniscal horns. This is thought to represent normal vasculature, seen in the meniscus of a child. This disappears in adulthood.
Regarding the meniscofemoral ligaments, either the anterior or posterior ligament is present on 33% of MRIs. Both ligaments are present on 3% of examinations. One of the 2 ligaments predominates. The ligament of Humphry is best seen on sagittal images. It is occasionally seen on coronal images. The ligament of Wrisberg is best seen on posterior coronal images.[23, 24]
Meniscal degeneration
Local increases in the degree of freedom of trapped water molecules within the substance of the meniscus occurs with age, resulting in increased T2 times. The appearance is that of increased signal intensity within the substance of the meniscus on short-TE images.[22]
Hello,
ReplyDeleteI’ve bookmarked your blog just now and I’ll be back to read more in the future my friend! Also nice colors on the layout, it’s really easy on the eyes.
Knee arthroscopy
DirectMed Part has more than 20 years of experience in providing medical imaging equipment as well as service market. Do not think more if you wish to purchase Refurbished MRI machine because you can also get it from this place.
ReplyDeletehttp://www.directmedparts.com/