Overview
According
to the 1992 International Symposium on Acute Pancreatitis, acute
pancreatitis is defined as an acute inflammatory process of the pancreas
with variable involvement of other regional tissues or remote organ
systems (see the image below).[1] Acute
pancreatitis is classified further into mild and severe forms. Mild
acute pancreatitis is associated with minimal organ dysfunction and
uneventful recovery. Severe acute pancreatitis is associated with
pancreatic necrosis and may lead to organ failure and/or local
complications.[2, 3, 4]
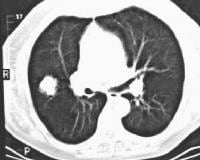
 Acute
pancreatitis. Focal pancreatitis involving pancreatic head. Pancreatic
head is enlarged with adjacent ill-defined peripancreatic inflammation
and fluid collections. Local complications of acute
pancreatitis include fluid collections, pseudocyst formation, abscess,
pancreatic necrosis, hemorrhage, venous thrombosis, and pseudoaneurysm
formation (see the images below).[5] A
pseudocyst is defined as a collection of pancreatic juice enclosed by a
wall of fibrous or granulation tissue. A pseudocyst lacks a true
epithelial lining and often communicates with the pancreatic duct. A
pancreatic abscess is a circumscribed intra-abdominal collection of pus.
The development of both pseudocyst and abscess usually requires 4 or
more weeks from the initial clinical onset of acute pancreatitis.[6] Pancreatic
necrosis is defined as focal or diffuse areas of nonviable pancreatic
parenchyma; it usually is associated with peripancreatic fat necrosis.
Necrosis usually develops early in the course of acute pancreatitis.[7]
Acute
pancreatitis. Focal pancreatitis involving pancreatic head. Pancreatic
head is enlarged with adjacent ill-defined peripancreatic inflammation
and fluid collections. Local complications of acute
pancreatitis include fluid collections, pseudocyst formation, abscess,
pancreatic necrosis, hemorrhage, venous thrombosis, and pseudoaneurysm
formation (see the images below).[5] A
pseudocyst is defined as a collection of pancreatic juice enclosed by a
wall of fibrous or granulation tissue. A pseudocyst lacks a true
epithelial lining and often communicates with the pancreatic duct. A
pancreatic abscess is a circumscribed intra-abdominal collection of pus.
The development of both pseudocyst and abscess usually requires 4 or
more weeks from the initial clinical onset of acute pancreatitis.[6] Pancreatic
necrosis is defined as focal or diffuse areas of nonviable pancreatic
parenchyma; it usually is associated with peripancreatic fat necrosis.
Necrosis usually develops early in the course of acute pancreatitis.[7]
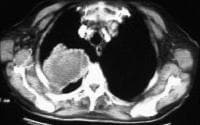
 Acute
pancreatitis. Pancreatic abscess. Large, relatively well-circumscribed
heterogeneous collection containing gas bubbles inferior to the
pancreatic head. This collection was drained successfully and
percutaneously via a 12Fr pigtail catheter.
Acute
pancreatitis. Pancreatic abscess. Large, relatively well-circumscribed
heterogeneous collection containing gas bubbles inferior to the
pancreatic head. This collection was drained successfully and
percutaneously via a 12Fr pigtail catheter.  Acute
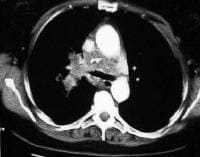
pancreatitis. Pancreatic necrosis. Note the nonenhancing pancreatic
body anterior to the splenic vein. Also present is peripancreatic fluid
extending anteriorly from the pancreatic head.
Acute
pancreatitis. Pancreatic necrosis. Note the nonenhancing pancreatic
body anterior to the splenic vein. Also present is peripancreatic fluid
extending anteriorly from the pancreatic head.  Acute
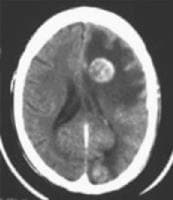
pancreatitis. Pancreatic necrosis. Approximately 50% of the pancreatic
gland does not display enhancement after contrast administration. Gallstones
and alcohol abuse are the most common causes of acute pancreatitis,
accounting for 60-80% of cases. Other causes include blunt trauma to the
abdomen, iatrogenic trauma (postoperative trauma, endoscopic retrograde
cholangiopancreatography), hypertriglyceridemia, hypercalcemia,
drug-induced, infectious etiologies (eg, mumps, cytomegalovirus),
congenital anomalies (pancreas divisum, choledochocele), ampullary or
pancreatic tumors, vascular abnormalities (atherosclerotic emboli,
hypoperfusion, vasculitis), cystic fibrosis, and Reye syndrome. These
miscellaneous causes account for approximately 10% of cases of acute
pancreatitis. In approximately 10-25% of patients, no underlying cause
is found.[8, 9, 10]
Acute
pancreatitis. Pancreatic necrosis. Approximately 50% of the pancreatic
gland does not display enhancement after contrast administration. Gallstones
and alcohol abuse are the most common causes of acute pancreatitis,
accounting for 60-80% of cases. Other causes include blunt trauma to the
abdomen, iatrogenic trauma (postoperative trauma, endoscopic retrograde
cholangiopancreatography), hypertriglyceridemia, hypercalcemia,
drug-induced, infectious etiologies (eg, mumps, cytomegalovirus),
congenital anomalies (pancreas divisum, choledochocele), ampullary or
pancreatic tumors, vascular abnormalities (atherosclerotic emboli,
hypoperfusion, vasculitis), cystic fibrosis, and Reye syndrome. These
miscellaneous causes account for approximately 10% of cases of acute
pancreatitis. In approximately 10-25% of patients, no underlying cause
is found.[8, 9, 10]
CECT allows complete visualization of the pancreas and retroperitoneum, even in the setting of ileus or overlying bandages from a recent surgical procedure. CECT can help detect almost all major abdominal complications of acute pancreatitis, such as fluid collections, pseudocysts, abscesses, venous thrombosis, and pseudoaneurysms. In addition, CECT can be used to guide percutaneous/interventional procedures such as diagnostic fine-needle aspiration or catheter placement. CECT may be performed on severely ill patients including intubated patients. Lastly, CECT can be used as a prognostic indicator of the severity of acute pancreatitis.
Other adjunctive imaging modalities include ultrasonography (US), MRI, and angiography. US is especially useful in the diagnosis of gallstones and follow-up observation of pseudocysts. US also can be used to detect pancreatic pseudoaneurysms. The diagnostic efficacy of MRI is comparable to that of CECT, although MRI examination is more time consuming and costly.[11, 12, 13] Angiography is primarily used to help diagnose the vascular complications of acute pancreatitis.[14, 15, 16, 17, 18]
CT and US are the guidance modalities of choice in performing diagnostic fine-needle aspiration and percutaneous drainage of fluid collections. Diagnostic fine-needle aspiration is performed to distinguish infected from noninfected pseudocysts and to delineate pancreatic abscess from infected necrosis. The aspirate should be sent at once for Gram stain and subsequent aerobic, anaerobic, and fungal cultures. Treatment regimens for these entities differ.[19, 20]
In addition, CECT is far less sensitive than US in detecting gallstones or biliary duct stones, a common cause of acute pancreatitis. Therefore, if gallstones or an impacted common bile duct stone is not seen on CT, US is necessary to document the presence or absence of gallstones.
Acute
pancreatitis. Focal pancreatitis involving pancreatic head. Pancreatic
head is enlarged with adjacent ill-defined peripancreatic inflammation
and fluid collections. Local complications of acute
pancreatitis include fluid collections, pseudocyst formation, abscess,
pancreatic necrosis, hemorrhage, venous thrombosis, and pseudoaneurysm
formation (see the images below).[5] A
pseudocyst is defined as a collection of pancreatic juice enclosed by a
wall of fibrous or granulation tissue. A pseudocyst lacks a true
epithelial lining and often communicates with the pancreatic duct. A
pancreatic abscess is a circumscribed intra-abdominal collection of pus.
The development of both pseudocyst and abscess usually requires 4 or
more weeks from the initial clinical onset of acute pancreatitis.[6] Pancreatic
necrosis is defined as focal or diffuse areas of nonviable pancreatic
parenchyma; it usually is associated with peripancreatic fat necrosis.
Necrosis usually develops early in the course of acute pancreatitis.[7] Acute
pancreatitis. Pancreatic abscess. Large, relatively well-circumscribed
heterogeneous collection containing gas bubbles inferior to the
pancreatic head. This collection was drained successfully and
percutaneously via a 12Fr pigtail catheter. Acute
pancreatitis. Pancreatic necrosis. Note the nonenhancing pancreatic
body anterior to the splenic vein. Also present is peripancreatic fluid
extending anteriorly from the pancreatic head. Acute
pancreatitis. Pancreatic necrosis. Approximately 50% of the pancreatic
gland does not display enhancement after contrast administration. Gallstones
and alcohol abuse are the most common causes of acute pancreatitis,
accounting for 60-80% of cases. Other causes include blunt trauma to the
abdomen, iatrogenic trauma (postoperative trauma, endoscopic retrograde
cholangiopancreatography), hypertriglyceridemia, hypercalcemia,
drug-induced, infectious etiologies (eg, mumps, cytomegalovirus),
congenital anomalies (pancreas divisum, choledochocele), ampullary or
pancreatic tumors, vascular abnormalities (atherosclerotic emboli,
hypoperfusion, vasculitis), cystic fibrosis, and Reye syndrome. These
miscellaneous causes account for approximately 10% of cases of acute
pancreatitis. In approximately 10-25% of patients, no underlying cause
is found.[8, 9, 10] Preferred examination
Contrast-enhanced computed tomography (CECT) is the standard imaging modality for the evaluation of acute pancreatitis and its complications. Using non–contrast-enhanced CT, clinicians can establish the diagnosis and demonstrate fluid collections but cannot evaluate for pancreatic necrosis or vascular complications.CECT allows complete visualization of the pancreas and retroperitoneum, even in the setting of ileus or overlying bandages from a recent surgical procedure. CECT can help detect almost all major abdominal complications of acute pancreatitis, such as fluid collections, pseudocysts, abscesses, venous thrombosis, and pseudoaneurysms. In addition, CECT can be used to guide percutaneous/interventional procedures such as diagnostic fine-needle aspiration or catheter placement. CECT may be performed on severely ill patients including intubated patients. Lastly, CECT can be used as a prognostic indicator of the severity of acute pancreatitis.
Other adjunctive imaging modalities include ultrasonography (US), MRI, and angiography. US is especially useful in the diagnosis of gallstones and follow-up observation of pseudocysts. US also can be used to detect pancreatic pseudoaneurysms. The diagnostic efficacy of MRI is comparable to that of CECT, although MRI examination is more time consuming and costly.[11, 12, 13] Angiography is primarily used to help diagnose the vascular complications of acute pancreatitis.[14, 15, 16, 17, 18]
CT and US are the guidance modalities of choice in performing diagnostic fine-needle aspiration and percutaneous drainage of fluid collections. Diagnostic fine-needle aspiration is performed to distinguish infected from noninfected pseudocysts and to delineate pancreatic abscess from infected necrosis. The aspirate should be sent at once for Gram stain and subsequent aerobic, anaerobic, and fungal cultures. Treatment regimens for these entities differ.[19, 20]
Limitations of techniques
The usefulness of CECT is limited in patients who are allergic to intravenous (IV) contrast or have renal insufficiency. Patients who have severe acute pancreatitis often require multiple scans to assess progress and/or complications. This necessitates significant radiation doses.In addition, CECT is far less sensitive than US in detecting gallstones or biliary duct stones, a common cause of acute pancreatitis. Therefore, if gallstones or an impacted common bile duct stone is not seen on CT, US is necessary to document the presence or absence of gallstones.
Radiography
Plain films of the abdomen are part of the initial diagnostic workup of acute abdominal pain.[21] Findings
on plain films are nonspecific but are suggestive of acute
pancreatitis. The most commonly recognized radiologic signs associated
with acute pancreatitis include the following:
- Air in the duodenal C-loop
- The sentinel loop sign, which represents a focal dilated proximal jejunal loop in the left upper quadrant
- The colon cutoff sign, which represents distention of the colon to the transverse colon with a paucity of gas distal to the splenic flexure
Computed Tomography
CECT
scanning of the abdomen and pelvis is the standard imaging modality for
evaluating acute pancreatitis and its complications. Both IV and oral
contrast should be administered. Imaging protocols vary, but the most
important unifying point is to obtain thin-section images during the
peak of pancreatic arterial perfusion. This usually can be acquired by
imaging 30-40 seconds after the administration of iodinated contrast at
3-4 mL/s using helical CT. Some advocate the use of water as a negative
contrast agent, because barium in the duodenal sweep could potentially
obscure a high-attenuation stone. (See the image below.)
Acute
pancreatitis. Pancreatic necrosis. Note the nonenhancing pancreatic
body anterior to the splenic vein. Also present is peripancreatic fluid
extending anteriorly from the pancreatic head. Freeny recommends obtaining CECT in the following situations[23] :
Complications of acute pancreatitis, such as pseudocysts, abscess, necrosis, venous thrombosis, pseudoaneurysms, and hemorrhage, can be recognized with CECT.[24]
A pseudocyst appears as an oval or round water density collection with a thin or thick wall, which may enhance.
A pancreatic abscess can manifest as a thick-walled low-attenuation fluid collection with gas bubbles or a poorly defined fluid collection with mixed densities/attenuation. Gas bubbles are not specific for infection, and the diagnosis of a pancreatic abscess usually requires percutaneous fine-needle aspiration to confirm the presence of pus.
Necrotic pancreatic tissue is recognized by its failure to enhance after IV contrast administration. Balthazar et al point out that the normal unenhanced pancreas has CT attenuation measuring 30-50 Hounsfield units (HU) and that after IV contrast, the pancreas should display attenuation measuring 100-150 HU.[25] A focal or diffuse well-marginated zone of unenhanced parenchyma (>3 cm in diameter or >30% of pancreatic area) is considered a reliable CT finding for the diagnosis of necrosis. It should be noted that pancreatic necrosis may be radiologically indistinguishable from a pancreatic abscess.
Venous thrombosis can be identified through a failure of the peripancreatic vein (eg, splenic vein, portal vein) to enhance or as an intraluminal filling defect.
Associated gastric varices may be identified.
A pseudoaneurysm usually appears as a well-defined round structure with a contrast-enhancement pattern similar to that of the aorta and other arteries. Hemorrhage appears as high-attenuation fluid collections. Active bleeding is seen as contrast extravasation.
CECT can be used to assess the severity of acute pancreatitis and to estimate the prognosis. Balthazar et al developed a grading system in which patients with acute pancreatitis are classified into 1 of the following 5 grades[25] :
Balthazar et al further constructed a CT severity index (CTSI) for acute pancreatitis that combines the grade of pancreatitis with the extent of pancreatic necrosis.[25] The CTSI assigns points to patients according to their grade of acute pancreatitis as well as the degree of pancreatic necrosis. More points are given for a higher grade of pancreatitis and for more extensive necrosis. Patients with a CTSI of 0-3 had a mortality of 3% and a complication rate of 8%. Patients with a CTSI of 4-6 had a mortality rate of 6% and a complication rate of 35%. Patients with a CTSI of 7-10 had a 17% mortality rate and a 92% complication rate.
Grade of acute pancreatis and the points assigned per grade are as follows:
Acute
pancreatitis. Pancreatic necrosis. Note the nonenhancing pancreatic
body anterior to the splenic vein. Also present is peripancreatic fluid
extending anteriorly from the pancreatic head. Freeny recommends obtaining CECT in the following situations[23] :- Patients in whom the clinical diagnosis is in doubt
- Patients with hyperamylasemia and severe clinical pancreatitis, abdominal distention, tenderness, high fever, and leukocytosis
- Patients with a Ranson score greater than 3 or an APACHE score greater than 8
- Patients who do not manifest rapid clinical improvement within 72 hours of initiation of conservative medical therapy
- Patients who demonstrate clinical improvement during initial medical therapy but then manifest an acute change in clinical status, indicating a developing complication
Complications of acute pancreatitis, such as pseudocysts, abscess, necrosis, venous thrombosis, pseudoaneurysms, and hemorrhage, can be recognized with CECT.[24]
A pseudocyst appears as an oval or round water density collection with a thin or thick wall, which may enhance.
A pancreatic abscess can manifest as a thick-walled low-attenuation fluid collection with gas bubbles or a poorly defined fluid collection with mixed densities/attenuation. Gas bubbles are not specific for infection, and the diagnosis of a pancreatic abscess usually requires percutaneous fine-needle aspiration to confirm the presence of pus.
Necrotic pancreatic tissue is recognized by its failure to enhance after IV contrast administration. Balthazar et al point out that the normal unenhanced pancreas has CT attenuation measuring 30-50 Hounsfield units (HU) and that after IV contrast, the pancreas should display attenuation measuring 100-150 HU.[25] A focal or diffuse well-marginated zone of unenhanced parenchyma (>3 cm in diameter or >30% of pancreatic area) is considered a reliable CT finding for the diagnosis of necrosis. It should be noted that pancreatic necrosis may be radiologically indistinguishable from a pancreatic abscess.
Venous thrombosis can be identified through a failure of the peripancreatic vein (eg, splenic vein, portal vein) to enhance or as an intraluminal filling defect.
Associated gastric varices may be identified.
A pseudoaneurysm usually appears as a well-defined round structure with a contrast-enhancement pattern similar to that of the aorta and other arteries. Hemorrhage appears as high-attenuation fluid collections. Active bleeding is seen as contrast extravasation.
CECT can be used to assess the severity of acute pancreatitis and to estimate the prognosis. Balthazar et al developed a grading system in which patients with acute pancreatitis are classified into 1 of the following 5 grades[25] :
- Grade A - Normal-appearing pancreas
- Grade B - Focal or diffuse enlargement of the pancreas
- Grade C - Pancreatic gland abnormalities associated with peripancreatic fat infiltration
- Grade D - A single fluid collection
- Grade E - Two or more fluid collections
Balthazar et al further constructed a CT severity index (CTSI) for acute pancreatitis that combines the grade of pancreatitis with the extent of pancreatic necrosis.[25] The CTSI assigns points to patients according to their grade of acute pancreatitis as well as the degree of pancreatic necrosis. More points are given for a higher grade of pancreatitis and for more extensive necrosis. Patients with a CTSI of 0-3 had a mortality of 3% and a complication rate of 8%. Patients with a CTSI of 4-6 had a mortality rate of 6% and a complication rate of 35%. Patients with a CTSI of 7-10 had a 17% mortality rate and a 92% complication rate.
Grade of acute pancreatis and the points assigned per grade are as follows:
- Grade A - 0 points
- Grade B - 1 point
- Grade C - 2 points
- Grade D - 3 points
- Grade E - 4 points
- None - 0 points
- Grade 0.33 - 2 points
- Grade 0.5 - 4 points
- Grade higher than 0.5 - 6 points
Degree of confidence
In a prospective study of 202 patients, Clavien et al reported a 92% sensitivity and 100% specificity in diagnosing acute pancreatitis via CECT.[26] Balthazar et al reported an overall accuracy of 80-90% in the detection of pancreatic necrosis.[25] Small areas of necrosis involving less than 30% of the pancreas can be missed. Nevertheless, the extent of pancreatic necrosis has been found to correlate well with operative findings and clinical severity. In a study by Block et al, the positive predictive value of CECT for pancreatic necrosis was found to be 92%.[27]False positives/negatives
The pancreas may appear normal in approximately 25% of patients with mild pancreatitis. In the acute phase of pancreatitis, a small number of patients will have a false-positive diagnosis for necrosis due to massive interstitial edema and vasoconstriction of the vascular arcades. Repeat CT within a few days may show normal pancreatic enhancement.Magnetic Resonance Imaging
Although
CT has long been the mainstay for imaging acute pancreatitis and its
complications, MRI is an excellent alternative imaging modality.[28, 29, 30] MRI
is a viable alternative in situations in which CECT is contraindicated,
such as in patients with contrast allergy or renal insufficiency. (See
the images below.)
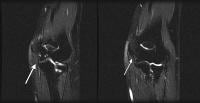
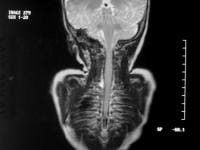
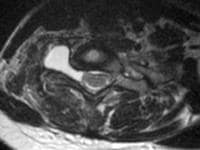
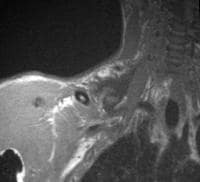
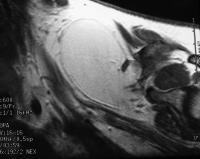
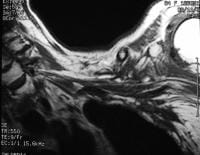
Acute
pancreatitis. Focal pancreatitis involving pancreatic head. Pancreatic
head is enlarged with adjacent ill-defined peripancreatic inflammation
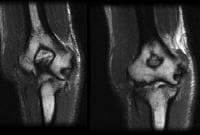
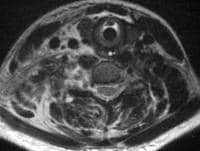
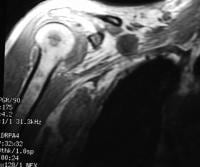
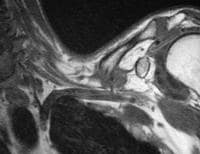
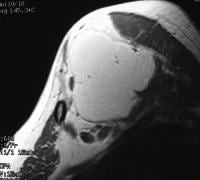
and fluid collections. Acute
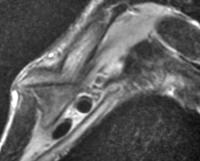
pancreatitis. Pancreatic abscess. Large, relatively well-circumscribed
heterogeneous collection containing gas bubbles inferior to the
pancreatic head. This collection was drained successfully and
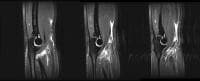
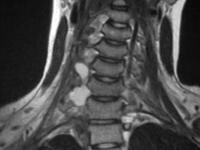
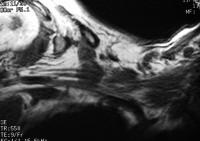
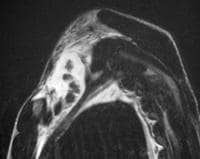
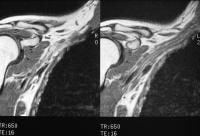
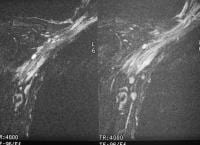
percutaneously via a 12Fr pigtail catheter. Acute
pancreatitis. Pancreatic necrosis. Approximately 50% of the pancreatic
gland does not display enhancement after contrast administration. In
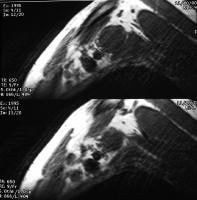
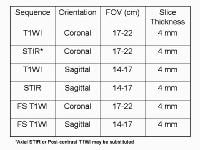
addition to T1-weighted and fast spin-echo T2-weighted sequences,
2-dimensional Fourier transform (FT) and 3-dimensional FT gradient-echo
sequences can be used to rapidly image the pancreas during patient
breath holds; this reduces the artifacts related to physiologic motion.
Bolus contrast administration of gadolinium chelates can be used to assess for pancreatic necrosis. The quality of upper abdominal imaging is enhanced further with the use of phased-array surface coils and fat-suppression techniques.
Detrimental effects of physiologic motion can be reduced further using ultrafast T2-weighted sequences, such as single-shot fast spin-echo or half-Fourier acquisition single-shot turbo-spin echo (HASTE) sequences. Subsecond image acquisitions provide quality diagnostic images even in uncooperative or tachypneic patients. These sequences also are used routinely for depicting the biliary tract in magnetic resonance cholangiopancreatography (MRCP). The normal pancreas demonstrates relatively high signal intensity on T1-weighted images with fat suppression.
The morphologic changes of acute pancreatitis are similar on CT and MRI.
The pancreas may be enlarged focally (usually the pancreatic head) or diffusely. Acute inflammatory changes appear as strands of low signal intensity in the surrounding peripancreatic fat.
Complications of acute pancreatitis also can be identified. Hemorrhage is characterized by T1 shortening or high signal intensity on T1-weighted sequences with fat suppression. Peripancreatic fluid collections, pseudocysts, and abscesses are recognized by their high signal intensity on T2-weighted sequences. Devascularized or necrotic portions of the pancreas fail to enhance on dynamic gadolinium-enhanced images. MRI also may be better than CT in detecting areas of sterile pancreatic necrosis in what appear to be simple pseudocysts on CT.
Gadolinium-based contrast agents (gadopentetate dimeglumine [Magnevist], gadobenate dimeglumine [MultiHance], gadodiamide [Omniscan], gadoversetamide [OptiMARK], gadoteridol [ProHance]) have recently been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). For more information, see the eMedicine topic Nephrogenic Systemic Fibrosis. The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans.
As of late December 2006, the FDA had received reports of 90 such cases of NSF/NFD . Worldwide, over 200 cases have been reported, according to the FDA. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Acute
pancreatitis. Focal pancreatitis involving pancreatic head. Pancreatic
head is enlarged with adjacent ill-defined peripancreatic inflammation
and fluid collections. Acute
pancreatitis. Pancreatic abscess. Large, relatively well-circumscribed
heterogeneous collection containing gas bubbles inferior to the
pancreatic head. This collection was drained successfully and
percutaneously via a 12Fr pigtail catheter. Acute
pancreatitis. Pancreatic necrosis. Approximately 50% of the pancreatic
gland does not display enhancement after contrast administration. In
addition to T1-weighted and fast spin-echo T2-weighted sequences,
2-dimensional Fourier transform (FT) and 3-dimensional FT gradient-echo
sequences can be used to rapidly image the pancreas during patient
breath holds; this reduces the artifacts related to physiologic motion. Bolus contrast administration of gadolinium chelates can be used to assess for pancreatic necrosis. The quality of upper abdominal imaging is enhanced further with the use of phased-array surface coils and fat-suppression techniques.
Detrimental effects of physiologic motion can be reduced further using ultrafast T2-weighted sequences, such as single-shot fast spin-echo or half-Fourier acquisition single-shot turbo-spin echo (HASTE) sequences. Subsecond image acquisitions provide quality diagnostic images even in uncooperative or tachypneic patients. These sequences also are used routinely for depicting the biliary tract in magnetic resonance cholangiopancreatography (MRCP). The normal pancreas demonstrates relatively high signal intensity on T1-weighted images with fat suppression.
The morphologic changes of acute pancreatitis are similar on CT and MRI.
The pancreas may be enlarged focally (usually the pancreatic head) or diffusely. Acute inflammatory changes appear as strands of low signal intensity in the surrounding peripancreatic fat.
Complications of acute pancreatitis also can be identified. Hemorrhage is characterized by T1 shortening or high signal intensity on T1-weighted sequences with fat suppression. Peripancreatic fluid collections, pseudocysts, and abscesses are recognized by their high signal intensity on T2-weighted sequences. Devascularized or necrotic portions of the pancreas fail to enhance on dynamic gadolinium-enhanced images. MRI also may be better than CT in detecting areas of sterile pancreatic necrosis in what appear to be simple pseudocysts on CT.
Gadolinium-based contrast agents (gadopentetate dimeglumine [Magnevist], gadobenate dimeglumine [MultiHance], gadodiamide [Omniscan], gadoversetamide [OptiMARK], gadoteridol [ProHance]) have recently been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). For more information, see the eMedicine topic Nephrogenic Systemic Fibrosis. The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans.
As of late December 2006, the FDA had received reports of 90 such cases of NSF/NFD . Worldwide, over 200 cases have been reported, according to the FDA. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Degree of confidence
In a small study by Saifuddin et al, MRI was found to be equivalent to CECT in helping assess the location and extent of peripancreatic inflammatory changes and fluid collections.[31] In addition, MRI was found to be equivalent in helping assess the degree of pancreatic necrosis. Chalmers et al showed that MRI is more effective than CECT in helping characterize the content of fluid collections and in helping demonstrate gallstones.[32]False positives/negatives
In mild cases of acute pancreatitis, the pancreas can appear completely normal on MRI. MRI also is limited in detecting gas and calcifications.Ultrasonography
Jeffrey
recommends obtaining images of the pancreas and the peripancreatic
compartments, such as the lesser sac, anterior pararenal space, and
transverse mesocolon, by scanning in the supine, longitudinal,
transverse, semi-erect, and coronal planes.[33, 34, 35] However, regions of the pancreas may not be visible by US because of overlying bowel gas.
The spleen can be used as an acoustic window to image the pancreatic tail.
Laing et al advise radiologists to scrutinize the intrapancreatic portion of the common bile duct carefully for biliary stones.[36]
Doppler techniques should be used to assess vascular complications of acute pancreatitis, such as venous thrombosis and pseudoaneurysm formation.
US is the most sensitive modality for concomitantly evaluating the biliary tree/gallbladder.
More definitive findings include a diffusely enlarged hypoechoic gland. Focal enlargement of the pancreatic head and body also may be seen.
Complications of acute pancreatitis may be identified. Peripancreatic free fluid collections are identified as ill-defined anechoic collections. The fluid collections may demonstrate internal echoes/debris or septations if hemorrhage or a superimposed infection has occurred.
Extrapancreatic spread of acute pancreatitis may be the only sonographic manifestation of acute pancreatitis in some patients.
Pseudocysts appear as well-defined round or oval anechoic fluid collections with through transmission. Infected and noninfected pseudocysts are indistinguishable from each other sonographically. US often is used to monitor the resolution of pancreatic pseudocysts.
A pancreatic abscess may appear as a complex cystic structure with internal debris/septations and, possibly, echogenic gas bubbles. A pseudoaneurysm often appears as a cystic mass with turbulent arterial flow within the mass.
Acute hemorrhage may be identified as a hyperechoic fluid collection. Venous thrombosis can be identified as an intraluminal filling defect. Associated gastric varices may be appreciated.
The spleen can be used as an acoustic window to image the pancreatic tail.
Laing et al advise radiologists to scrutinize the intrapancreatic portion of the common bile duct carefully for biliary stones.[36]
Doppler techniques should be used to assess vascular complications of acute pancreatitis, such as venous thrombosis and pseudoaneurysm formation.
US is the most sensitive modality for concomitantly evaluating the biliary tree/gallbladder.
More definitive findings include a diffusely enlarged hypoechoic gland. Focal enlargement of the pancreatic head and body also may be seen.
Complications of acute pancreatitis may be identified. Peripancreatic free fluid collections are identified as ill-defined anechoic collections. The fluid collections may demonstrate internal echoes/debris or septations if hemorrhage or a superimposed infection has occurred.
Extrapancreatic spread of acute pancreatitis may be the only sonographic manifestation of acute pancreatitis in some patients.
Pseudocysts appear as well-defined round or oval anechoic fluid collections with through transmission. Infected and noninfected pseudocysts are indistinguishable from each other sonographically. US often is used to monitor the resolution of pancreatic pseudocysts.
A pancreatic abscess may appear as a complex cystic structure with internal debris/septations and, possibly, echogenic gas bubbles. A pseudoaneurysm often appears as a cystic mass with turbulent arterial flow within the mass.
Acute hemorrhage may be identified as a hyperechoic fluid collection. Venous thrombosis can be identified as an intraluminal filling defect. Associated gastric varices may be appreciated.
Degree of confidence
A primary limitation of US is that often the pancreas cannot be visualized secondary to overlying bowel gas. Neoptolemos et al report a sensitivity of 67% and a specificity of 100% in the diagnosis of acute pancreatitis by US.[37]False positives/negatives
The pancreas may appear completely normal in mild cases of acute pancreatitis.Angiography
Vascular
complications of acute pancreatitis result from the proteolytic effects
of the pancreatic enzymes that cause erosion of blood vessels, which
often results in pseudoaneurysm formation or free rupture. The splenic
artery, followed by the pancreaticoduodenal and gastroduodenal arteries,
are affected most commonly. The left gastric, hepatic, and small
intrapancreatic arteries are involved less often.
If acute hemorrhage or pseudoaneurysm is suspected or diagnosed by US or CECT, a celiac/superior mesenteric arteriogram should be performed to definitively assess the extent of vascular involvement. In addition, permanent or temporary therapeutic embolization can be performed. The primary contraindication for angiography is a hemodynamically unstable patient.
The precise bleeding point is identified by noting free contrast extravasation. Once the site of pseudoaneurysm or the source of active bleeding is identified, it can be treated by Gelfoam embolization, various coil occlusion devices, or tissue adhesives (eg, bucrylate). Superselective microcoil embolization also has been advocated by Reber et al.[38] Vujic has suggested using small Gelfoam particles to control diffuse pancreatic surface bleeding.[39] Diffuse bleeding from the gland may appear angiographically as a prominent blush.
Vujic reports that embolization may be used as a temporizing measure to slow bleeding so that the patient may be operated on electively.[39] This temporary therapeutic procedure involves selective or nonselective Gelfoam embolization or balloon occlusion of the main celiac trunk.
Complications of celiac/superior mesenteric arteriography and embolization include arterial injury such as thrombosis, dissection, or rupture, distal embolization, ischemia of visceral organs such as the spleen and bowel, coil malpositioning, and rebleeding.
Venous thrombosis of the splenic vein and/or collateral venous pathways also may be diagnosed via selective angiography.
If acute hemorrhage or pseudoaneurysm is suspected or diagnosed by US or CECT, a celiac/superior mesenteric arteriogram should be performed to definitively assess the extent of vascular involvement. In addition, permanent or temporary therapeutic embolization can be performed. The primary contraindication for angiography is a hemodynamically unstable patient.
The precise bleeding point is identified by noting free contrast extravasation. Once the site of pseudoaneurysm or the source of active bleeding is identified, it can be treated by Gelfoam embolization, various coil occlusion devices, or tissue adhesives (eg, bucrylate). Superselective microcoil embolization also has been advocated by Reber et al.[38] Vujic has suggested using small Gelfoam particles to control diffuse pancreatic surface bleeding.[39] Diffuse bleeding from the gland may appear angiographically as a prominent blush.
Vujic reports that embolization may be used as a temporizing measure to slow bleeding so that the patient may be operated on electively.[39] This temporary therapeutic procedure involves selective or nonselective Gelfoam embolization or balloon occlusion of the main celiac trunk.
Complications of celiac/superior mesenteric arteriography and embolization include arterial injury such as thrombosis, dissection, or rupture, distal embolization, ischemia of visceral organs such as the spleen and bowel, coil malpositioning, and rebleeding.
Venous thrombosis of the splenic vein and/or collateral venous pathways also may be diagnosed via selective angiography.