Overview
Subdural
hematomas (SDH) are 1 of the 3 types of extra-axial intracranial
hemorrhages (along with subarachnoid and epidural hemorrhages) and
usually occur as a result of trauma. Deceleration injuries are often the
cause of subdural bleeding from rupturing of veins via a shearing
mechanism. Other entities, such as child abuse and ventricular
decompression, also can result in subdural bleeding, and spontaneous
hemorrhages may occur in patients receiving anticoagulants or patients
with a coagulopathy condition. Compression of a dural sinus does not
directly cause a subdural hematoma, although compression may result in a
venous infarction.
Some subdural hematomas are clinically silent, whereas others cause symptoms as a result of mass effect on the adjacent brain. Some hematomas can grow large enough to result in herniation of cerebral tissue. Before computed tomography (CT) scanning and magnetic resonance imaging (MRI) technology, subdural hematomas were diagnosed only on the basis of this mass effect, which was depicted as displacement of the blood vessels on angiograms or as a calcified pituitary gland on skull radiographs. The advent of CT scan and MRI studies has made the diagnosis of even small hemorrhages routine (see the image below).
 Axial
head computed tomography scan demonstrates a skull fracture with an
adjacent, small subdural hematoma. Window and level values are widened
over standard values, which aids in the detection of small hemorrhages.
Axial
head computed tomography scan demonstrates a skull fracture with an
adjacent, small subdural hematoma. Window and level values are widened
over standard values, which aids in the detection of small hemorrhages.
For excellent patient education resources, visit eMedicine's Brain and Nervous System Center. Also, see eMedicine's patient education articles Head Injury, Concussion, and Aneurysm, Brain.
Some subdural hematomas are clinically silent, whereas others cause symptoms as a result of mass effect on the adjacent brain. Some hematomas can grow large enough to result in herniation of cerebral tissue. Before computed tomography (CT) scanning and magnetic resonance imaging (MRI) technology, subdural hematomas were diagnosed only on the basis of this mass effect, which was depicted as displacement of the blood vessels on angiograms or as a calcified pituitary gland on skull radiographs. The advent of CT scan and MRI studies has made the diagnosis of even small hemorrhages routine (see the image below).
Axial
head computed tomography scan demonstrates a skull fracture with an
adjacent, small subdural hematoma. Window and level values are widened
over standard values, which aids in the detection of small hemorrhages. Preferred examination
CT scanning is usually the first evaluation in patients with suspected acute subdural hematoma because CT scans depict acute hemorrhage and skull fractures well, they are relatively fast to obtain, and CT scanning is more readily available than MRI. Smaller hemorrhages may be missed on CT scans, and in the nonacute setting, MRI is the study of choice because of its high sensitivity and specificity.[1, 2]Limitations of techniques
CT scanning may fail to depict small hemorrhages because of the similarity in attenuation between blood and adjacent bone and because of streak artifacts in the posterior fossa and inferior middle cranial fossa. MRI aids in the detection of small hematomas because of its multiplanar capabilities.For excellent patient education resources, visit eMedicine's Brain and Nervous System Center. Also, see eMedicine's patient education articles Head Injury, Concussion, and Aneurysm, Brain.
Computed Tomography
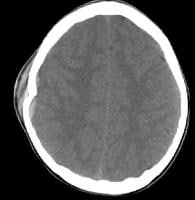
CT scan findings in subdural hematomas depend on the age of the hemorrhage (see the image below).[3, 4, 5]
 Computed
tomography (CT) scan demonstrating a patient with subdural hematomas of
varying ages. This patient had a CT scan 1 week prior that demonstrated
a chronic subdural hematoma (represented by the low density fluid on
this study). Over the next week, his clinical condition progressively
declined, then he collapsed shortly before this image was obtained. The
gray blood represents subacute hemorrhage, whereas the white blood
represents acute. In the acute phase, subdural hematomas
appear as a crescent-shaped extra-axial collection with increased
attenuation that, when large enough, causes effacement of the adjacent
sulci and midline shift. The attenuation changes as the hematoma ages
(see the images below).[6, 7]
Computed
tomography (CT) scan demonstrating a patient with subdural hematomas of
varying ages. This patient had a CT scan 1 week prior that demonstrated
a chronic subdural hematoma (represented by the low density fluid on
this study). Over the next week, his clinical condition progressively
declined, then he collapsed shortly before this image was obtained. The
gray blood represents subacute hemorrhage, whereas the white blood
represents acute. In the acute phase, subdural hematomas
appear as a crescent-shaped extra-axial collection with increased
attenuation that, when large enough, causes effacement of the adjacent
sulci and midline shift. The attenuation changes as the hematoma ages
(see the images below).[6, 7]
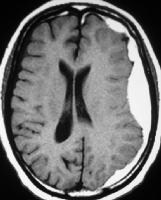
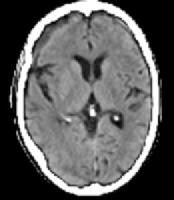 Late
subacute subdural hematoma has decreased attenuation compared with
adjacent brain tissue. Attenuation of the hematoma remains higher than
that of cerebrospinal fluid.
Late
subacute subdural hematoma has decreased attenuation compared with
adjacent brain tissue. Attenuation of the hematoma remains higher than
that of cerebrospinal fluid. 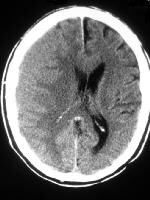 Computed
tomography scan in a patient with a subacute right frontal subdural
hematoma. The blood has the same attenuation as that of the adjacent
gray matter and is difficult to distinguish. Note that the gray
matter–white matter junction is displaced medially, and midline shift is
seen, indicating the presence of a space-occupying extra-axial lesion. Subacute
subdural hematomas may be difficult to detect because they may have
isoattenuation compared with adjacent gray matter. Displacement of the
gray matter–white matter junction is an important sign that indicates
the presence of a space-occupying lesion. Although often administered in
the past to help detect displacement of cortical vessels, contrast
medium is not necessary with the capabilities of current scanners.
Computed
tomography scan in a patient with a subacute right frontal subdural
hematoma. The blood has the same attenuation as that of the adjacent
gray matter and is difficult to distinguish. Note that the gray
matter–white matter junction is displaced medially, and midline shift is
seen, indicating the presence of a space-occupying extra-axial lesion. Subacute
subdural hematomas may be difficult to detect because they may have
isoattenuation compared with adjacent gray matter. Displacement of the
gray matter–white matter junction is an important sign that indicates
the presence of a space-occupying lesion. Although often administered in
the past to help detect displacement of cortical vessels, contrast
medium is not necessary with the capabilities of current scanners.
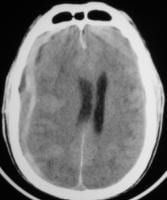
Chronic subdural hematomas (see the image below) have isoattenuation relative to the cerebrospinal fluid (CSF). In rare cases, such hematomas may calcify, resulting in an unusual appearance that can be mistaken for a calcified mass.
 Late subacute-to-chronic subdural hematoma with a blood-fluid level indicating acute hemorrhage into the chronic collection. Unlike
epidural hematomas, subdural hematomas are not restricted by dural
tethering at the cranial sutures; they can cross suture lines and
continue along the falx and tentorium (see the image below). However,
they do not cross the midline because of the meningeal reflections.
Late subacute-to-chronic subdural hematoma with a blood-fluid level indicating acute hemorrhage into the chronic collection. Unlike
epidural hematomas, subdural hematomas are not restricted by dural
tethering at the cranial sutures; they can cross suture lines and
continue along the falx and tentorium (see the image below). However,
they do not cross the midline because of the meningeal reflections.
 Tentorial subdural hematoma in an adult with trauma. In children with this pattern of injury, abuse should be considered. When
a subdural hematoma is discovered on a CT scan, it is important to
check for the presence of other related injuries, such as skull fracture
(see the first image below), intraparenchymal contusions, and
subarachnoid blood (see the second image below). The presence of
adjacent parenchymal injury in patients with a subdural hematoma is the
most important factor in predicting their clinical outcome.
Tentorial subdural hematoma in an adult with trauma. In children with this pattern of injury, abuse should be considered. When
a subdural hematoma is discovered on a CT scan, it is important to
check for the presence of other related injuries, such as skull fracture
(see the first image below), intraparenchymal contusions, and
subarachnoid blood (see the second image below). The presence of
adjacent parenchymal injury in patients with a subdural hematoma is the
most important factor in predicting their clinical outcome.
Axial
head computed tomography scan demonstrates a skull fracture with an
adjacent, small subdural hematoma. Window and level values are widened
over standard values, which aids in the detection of small hemorrhages. 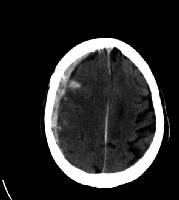 Subdural
hematoma with adjacent subarachnoid hemorrhage was the result of a
ruptured middle cerebral artery aneurysm. Aneurysms are unusual causes
of subdural hematomas. Rebleeding into subdural hematomas also
may occur and is depicted as a layer of high-attenuation hemorrhage
within a lower attenuation hematoma.
Subdural
hematoma with adjacent subarachnoid hemorrhage was the result of a
ruptured middle cerebral artery aneurysm. Aneurysms are unusual causes
of subdural hematomas. Rebleeding into subdural hematomas also
may occur and is depicted as a layer of high-attenuation hemorrhage
within a lower attenuation hematoma.
In older patients with cerebral atrophy, an appearance of bilateral frontal subdural hygromas may be seen when the patient is in the supine position. However, the lack of mass effect and the presence of general atrophy suggest that this appearance is merely the result of settling of the atrophic brain rather than a pathologic subdural collection. A similar finding can be seen in young children (benign enlargement of the subarachnoid space), which should resolve in the first few years of life (see the image below).
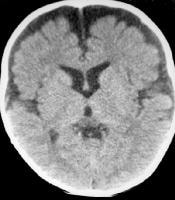 Axial
computed tomography scan demonstrates the benign enlargement of the
subarachnoid space that occurs in children. The extra-axial fluid does
not cause mass effect and normally resolves within the first 2 years of
life. Posttraumatic subdural hygromas can also be confused
with chronic subdural hematomas. These develop days or weeks following
trauma and result from tears in the arachnoid and resulting leakage of
CSF into the subdural space. They are self-limited and usually resolve
after several months.
Axial
computed tomography scan demonstrates the benign enlargement of the
subarachnoid space that occurs in children. The extra-axial fluid does
not cause mass effect and normally resolves within the first 2 years of
life. Posttraumatic subdural hygromas can also be confused
with chronic subdural hematomas. These develop days or weeks following
trauma and result from tears in the arachnoid and resulting leakage of
CSF into the subdural space. They are self-limited and usually resolve
after several months.
Computed
tomography (CT) scan demonstrating a patient with subdural hematomas of
varying ages. This patient had a CT scan 1 week prior that demonstrated
a chronic subdural hematoma (represented by the low density fluid on
this study). Over the next week, his clinical condition progressively
declined, then he collapsed shortly before this image was obtained. The
gray blood represents subacute hemorrhage, whereas the white blood
represents acute. In the acute phase, subdural hematomas
appear as a crescent-shaped extra-axial collection with increased
attenuation that, when large enough, causes effacement of the adjacent
sulci and midline shift. The attenuation changes as the hematoma ages
(see the images below).[6, 7] Late
subacute subdural hematoma has decreased attenuation compared with
adjacent brain tissue. Attenuation of the hematoma remains higher than
that of cerebrospinal fluid. Computed
tomography scan in a patient with a subacute right frontal subdural
hematoma. The blood has the same attenuation as that of the adjacent
gray matter and is difficult to distinguish. Note that the gray
matter–white matter junction is displaced medially, and midline shift is
seen, indicating the presence of a space-occupying extra-axial lesion. Subacute
subdural hematomas may be difficult to detect because they may have
isoattenuation compared with adjacent gray matter. Displacement of the
gray matter–white matter junction is an important sign that indicates
the presence of a space-occupying lesion. Although often administered in
the past to help detect displacement of cortical vessels, contrast
medium is not necessary with the capabilities of current scanners. Chronic subdural hematomas (see the image below) have isoattenuation relative to the cerebrospinal fluid (CSF). In rare cases, such hematomas may calcify, resulting in an unusual appearance that can be mistaken for a calcified mass.
Late subacute-to-chronic subdural hematoma with a blood-fluid level indicating acute hemorrhage into the chronic collection. Unlike
epidural hematomas, subdural hematomas are not restricted by dural
tethering at the cranial sutures; they can cross suture lines and
continue along the falx and tentorium (see the image below). However,
they do not cross the midline because of the meningeal reflections.Tentorial subdural hematoma in an adult with trauma. In children with this pattern of injury, abuse should be considered. When
a subdural hematoma is discovered on a CT scan, it is important to
check for the presence of other related injuries, such as skull fracture
(see the first image below), intraparenchymal contusions, and
subarachnoid blood (see the second image below). The presence of
adjacent parenchymal injury in patients with a subdural hematoma is the
most important factor in predicting their clinical outcome.Axial
head computed tomography scan demonstrates a skull fracture with an
adjacent, small subdural hematoma. Window and level values are widened
over standard values, which aids in the detection of small hemorrhages. Subdural
hematoma with adjacent subarachnoid hemorrhage was the result of a
ruptured middle cerebral artery aneurysm. Aneurysms are unusual causes
of subdural hematomas. Rebleeding into subdural hematomas also
may occur and is depicted as a layer of high-attenuation hemorrhage
within a lower attenuation hematoma.Degree of confidence
Differentiating subdural from epidural hematomas may be difficult when the hemorrhage is small, because the image of the blood may not demonstrate a typical shape in either condition. Follow-up imaging to ensure that the hematoma is not expanding and to check for an adjacent skull fracture is typical.False positives/negatives
Small subdural hematomas may not be depicted because the attenuation may be similar to the adjacent inner table of the skull. Viewing the images with a wider window and level (eg, 240 and 80 HU) assists in detection in these cases; however, CT scanning fails to depict a certain number of small hemorrhages. Gentry et al found that only 53% of acute and subacute subdural hematomas were revealed on CT scan studies compared with MRI; however, this study was performed using older CT technology.[8, 9]In older patients with cerebral atrophy, an appearance of bilateral frontal subdural hygromas may be seen when the patient is in the supine position. However, the lack of mass effect and the presence of general atrophy suggest that this appearance is merely the result of settling of the atrophic brain rather than a pathologic subdural collection. A similar finding can be seen in young children (benign enlargement of the subarachnoid space), which should resolve in the first few years of life (see the image below).
Axial
computed tomography scan demonstrates the benign enlargement of the
subarachnoid space that occurs in children. The extra-axial fluid does
not cause mass effect and normally resolves within the first 2 years of
life. Posttraumatic subdural hygromas can also be confused
with chronic subdural hematomas. These develop days or weeks following
trauma and result from tears in the arachnoid and resulting leakage of
CSF into the subdural space. They are self-limited and usually resolve
after several months. Magnetic Resonance Imaging
MRI
is more sensitive than CT scanning in the detection of subdural
hematomas because the multiplanar and superior tissue differentiation of
MRI makes detection easier. In particular, a sensitivity of more than
95% has been described with T2-weighted images of subdural hematomas
because of the marked difference in signal intensity between blood
products and adjacent structures (see the images below).
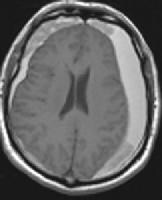 Axial
T1-weighted magnetic resonance imaging demonstrates bilateral subacute
subdural hematomas with increased signal intensity. Areas of
intermediate intensity represent more acute hemorrhage into the subacute
collections.
Axial
T1-weighted magnetic resonance imaging demonstrates bilateral subacute
subdural hematomas with increased signal intensity. Areas of
intermediate intensity represent more acute hemorrhage into the subacute
collections. 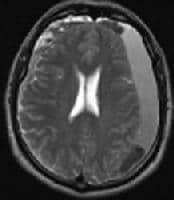 T2-weighted magnetic resonance imaging in a patient with subdural hematoma shows blood products of differing ages. The
shape of the subdural hematoma on axial images is the same
crescent-shaped pattern seen on CT scan images. Coronal images are
useful in evaluating the extent of subdural hematomas and in detecting
temporal and tentorial hemorrhages, 2 aspects that are poorly depicted
on CT scans.
T2-weighted magnetic resonance imaging in a patient with subdural hematoma shows blood products of differing ages. The
shape of the subdural hematoma on axial images is the same
crescent-shaped pattern seen on CT scan images. Coronal images are
useful in evaluating the extent of subdural hematomas and in detecting
temporal and tentorial hemorrhages, 2 aspects that are poorly depicted
on CT scans.
In subdural hematomas, the signal depends on the age of the hemorrhage and follows the signal pattern of intraparenchymal hematomas in acute and subacute cases (see the image below). Chronic subdural hematomas, which appear as isoattenuation relative to CSF on CT scans, often demonstrate increased signal intensity on T1-weighted images because of the presence of free methemoglobin, though the intensity decreases over time. Hemosiderin is usually not present and is believed to result from the lack of a dural blood–brain barrier.[10]
 Subacute
subdural hematoma with extension into the anterior interhemispheric
cistern. Note that the sutures do not contain the spread of these
hemorrhages. When hemorrhages of differing ages exist within a
subdural collection, septae may separate the different blood products
(see the first image below). In addition, a blood–fluid level may be
seen. When blood products of various ages are depicted on MRIs in a
child, particularly when the blood is at multiple sites, child abuse
must be suspected (see the second image below). Posterior
interhemispheric and tentorial subdural hematomas are also suggestive of
child abuse because they are associated with shaken baby syndrome.
Subacute
subdural hematoma with extension into the anterior interhemispheric
cistern. Note that the sutures do not contain the spread of these
hemorrhages. When hemorrhages of differing ages exist within a
subdural collection, septae may separate the different blood products
(see the first image below). In addition, a blood–fluid level may be
seen. When blood products of various ages are depicted on MRIs in a
child, particularly when the blood is at multiple sites, child abuse
must be suspected (see the second image below). Posterior
interhemispheric and tentorial subdural hematomas are also suggestive of
child abuse because they are associated with shaken baby syndrome.
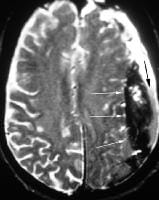 T2-weighted
magnetic resonance imaging in a patient with a subdural hematoma and
rebleeding clearly shows hemorrhages of 3 different ages; these are
hyperintense, isointense, and hypointense relative to brain tissue.
T2-weighted
magnetic resonance imaging in a patient with a subdural hematoma and
rebleeding clearly shows hemorrhages of 3 different ages; these are
hyperintense, isointense, and hypointense relative to brain tissue.
Axial
T1-weighted magnetic resonance imaging demonstrates bilateral subacute
subdural hematomas with increased signal intensity. Areas of
intermediate intensity represent more acute hemorrhage into the subacute
collections. T2-weighted magnetic resonance imaging in a patient with subdural hematoma shows blood products of differing ages. The
shape of the subdural hematoma on axial images is the same
crescent-shaped pattern seen on CT scan images. Coronal images are
useful in evaluating the extent of subdural hematomas and in detecting
temporal and tentorial hemorrhages, 2 aspects that are poorly depicted
on CT scans. In subdural hematomas, the signal depends on the age of the hemorrhage and follows the signal pattern of intraparenchymal hematomas in acute and subacute cases (see the image below). Chronic subdural hematomas, which appear as isoattenuation relative to CSF on CT scans, often demonstrate increased signal intensity on T1-weighted images because of the presence of free methemoglobin, though the intensity decreases over time. Hemosiderin is usually not present and is believed to result from the lack of a dural blood–brain barrier.[10]
Subacute
subdural hematoma with extension into the anterior interhemispheric
cistern. Note that the sutures do not contain the spread of these
hemorrhages. When hemorrhages of differing ages exist within a
subdural collection, septae may separate the different blood products
(see the first image below). In addition, a blood–fluid level may be
seen. When blood products of various ages are depicted on MRIs in a
child, particularly when the blood is at multiple sites, child abuse
must be suspected (see the second image below). Posterior
interhemispheric and tentorial subdural hematomas are also suggestive of
child abuse because they are associated with shaken baby syndrome.T2-weighted
magnetic resonance imaging in a patient with a subdural hematoma and
rebleeding clearly shows hemorrhages of 3 different ages; these are
hyperintense, isointense, and hypointense relative to brain tissue.
No comments:
Post a Comment