Magnetic resonance imaging (MRI) of the brain is useful in the diagnosis and treatment of multiple sclerosis
(MS), an inflammatory, demyelinating condition of the central nervous
system (CNS) that is generally considered to be autoimmune in nature.
White matter tracts are affected, including those of the cerebral
hemispheres, infratentorium, and spinal cord. MS lesions, known as
plaques, may form in CNS white matter in any location; thus, clinical
presentations may be diverse. Continuing lesion formation in MS often
leads to physical disability and, sometimes, to cognitive decline.
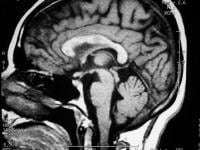 Sagittal
T1-weighted MRI depicts multiple hypointense lesions in the corpus
callosum; this finding is characteristic of multiple sclerosis.
Sagittal
T1-weighted MRI depicts multiple hypointense lesions in the corpus
callosum; this finding is characteristic of multiple sclerosis. 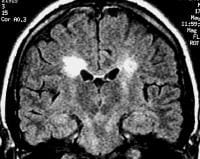 Coronal
fluid-attenuated inversion recovery (FLAIR) MRI in a patient with
multiple sclerosis demonstrates periventricular high–signal intensity
lesions, which exhibit a typical distribution for multiple sclerosis.
FLAIR MRI is a highly sensitive sequence for lesion detection,
particularly supratentorially.
Coronal
fluid-attenuated inversion recovery (FLAIR) MRI in a patient with
multiple sclerosis demonstrates periventricular high–signal intensity
lesions, which exhibit a typical distribution for multiple sclerosis.
FLAIR MRI is a highly sensitive sequence for lesion detection,
particularly supratentorially. 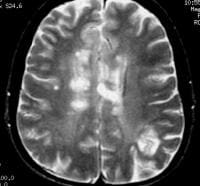 Axial
T2-weighted MRI in a patient with multiple sclerosis demonstrates
numerous white matter plaques in a callosal and pericallosal white
matter distribution.
Axial
T2-weighted MRI in a patient with multiple sclerosis demonstrates
numerous white matter plaques in a callosal and pericallosal white
matter distribution. 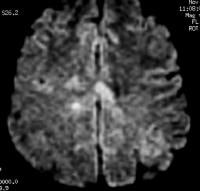 Axial
diffusion-weighted MRI in a patient with multiple sclerosis shows
several hyperintense lesions, a feature of inflammatory disease
activity. One of the limitations of using MRI in patients with
MS is the discordance occurring between lesion location and the
clinical presentation. In addition, depending on the number and location
of findings, MRI can vary greatly in terms of sensitivity and
specificity in the diagnosis of MS. This is especially true of primary
progressive MS, which may not show the classic discrete lesions of
relapsing-remitting MS.
Axial
diffusion-weighted MRI in a patient with multiple sclerosis shows
several hyperintense lesions, a feature of inflammatory disease
activity. One of the limitations of using MRI in patients with
MS is the discordance occurring between lesion location and the
clinical presentation. In addition, depending on the number and location
of findings, MRI can vary greatly in terms of sensitivity and
specificity in the diagnosis of MS. This is especially true of primary
progressive MS, which may not show the classic discrete lesions of
relapsing-remitting MS.
A clinician presented with an MRI report that details a few "nonspecific white matter lesions" that are "compatible with MS" is often frustrated with the lack of sensitivity and specificity of such a description. For this reason, imaging findings need to be described in detail, and preferably referenced to one of the published set of diagnostic criteria such as those by Paty[1] or Barkhof.[2] Finally, the specific patient's neurologic history and clinical findings must be correlated with the imaging to establish an accurate diagnosis.[3]
Plain radiographic studies have no positive predictive value in the diagnosis of multiple sclerosis, but occasionally, plain radiographs may be used to exclude mechanical bony lesions. Angiography also has a limited role in the diagnosis and management of MS, but when central nervous system (CNS) vasculitis is considered in a patient with undifferentiated findings, angiography may occasionally be considered.
Cerebrospinal fluid (CSF) analysis for oligoclonal banding or immunoglobulin G (IgG) levels is no longer routine in the investigation of MS, although this test may be of use when MRI is unavailable or MRI findings are nondiagnostic.[4]
Clinically, MS has historically been diagnosed via the demonstration of white matter dysfunction disseminated in time and space.[8] With the advent of diagnostic laboratory investigations and imaging techniques, the Poser criteria were proposed to establish a degree of certainty of diagnosis in the absence of the 2 clinical attacks by using terms such as possible MS and probable MS.[9]
With increasing treatment options for MS and better imaging techniques, newer diagnostic criteria have been suggested that allow diagnosis after a single attack coupled with appropriate positive test results. These criteria have been coined the MacDonald criteria.[10] Essentially, they allow for the second attack in time to be defined by a new lesion appearing on MRI. Also, the MacDonald criteria allow the dissemination in space to be established on the basis of either 9 typical white matter lesions on MRI or 1 enhancing lesion. If CSF studies show increased IgG values or oligoclonal banding, the presence of only 2 typical MRI lesions satisfy the dissemination-in-time criteria.
With respect to the initial clinical presentation in MS, it may vary with the white matter tract involved, and it may include somatic sensory changes, optic neuritis, or weakness, to mention just a few possible neurologic presentations. After only a single attack, the diagnosis of MS is suggested if the first impairment is coupled with positive paraclinical test results, such as those on imaging or CSF studies. Furthermore, the attack must be compatible with the pattern of impairment found in patients with MS, which typically means that the duration of deficit is days to weeks. Worsening of vision due to optic neuritis and subsequent exercise is known as the Uhthoff phenomenon.
Stankiewicz et al correlated brain lesions and clinical status with 1.5T and 3T MRI in 32 patients with MS by use of MRI fluid-attenuated inversion-recovery (FLAIR) sequences, and the authors found that MRI at 3T may provide increased sensitivity and validity in assessment of MS brain lesions. The study showed that FLAIR lesion volume (FLLV) at 3T was higher than at 1.5T. While 3T FLLV correlated moderately and significantly, 1.5T FLLV correlated poorly. When controlling for age and depression, correlations between FLLV and cognitive measures were significant at 1.5T for the Judgment of Line Orientation Test, the Symbol Digit Modalities Test, and the California Verbal Learning Test Delayed Free Recall, but at 3T, correlations were significant and of greater magnitude.[11]
Occasionally, the course of MS may be more indolent and exhibit a chronic, persistent neurologic deficit without apparent ongoing deterioration or further impairment. Sometimes, this course of MS is called inactive or benign MS, and this form is often observed in patients with prior relapsing-remitting disease.
Another potentially complicating matter clinically is that highly active MS lesions may sometimes demonstrate significant mass effect. Rarely, mass effect can lead to midline shift, herniations, infarctions, and even death. Such a drastic clinical and radiologic presentation can lead to an incorrect preliminary diagnosis and inappropriate neurosurgical intervention. When MS presents in a more fulminant, aggressive manner, it is frequently known as malignant MS or the Marburg variant.
In a prospective study, Lebrun et al followed 70 patients who had their first brain MRI for a variety of medical symptoms not suggestive of MS and found the mean time between the first brain MRI and the first clinically isolated syndrome to be 2.3 years (range, 0.8-5 y). Diagnostic studies of the blood, CSF, and visual evoked potentials were conducted, and clinical conversion occurred in 23 patients: 6 to optic neuritis, 6 to myelitis, 5 to brainstem symptoms, 4 to sensitive symptoms, 1 to cerebellar symptoms, and 1 to cognitive deterioration.[12] For patient education information, see Multiple Sclerosis.
Preferred examination
Radiologically, the use of MRI is revolutionizing the investigation, diagnosis, and even the treatment of MS (see the images below). Usually, MRI is the only imaging modality needed for imaging patients with MS, and it far surpasses all other tests with respect to its positive predictive value.Sagittal
T1-weighted MRI depicts multiple hypointense lesions in the corpus
callosum; this finding is characteristic of multiple sclerosis. Coronal
fluid-attenuated inversion recovery (FLAIR) MRI in a patient with
multiple sclerosis demonstrates periventricular high–signal intensity
lesions, which exhibit a typical distribution for multiple sclerosis.
FLAIR MRI is a highly sensitive sequence for lesion detection,
particularly supratentorially. Axial
T2-weighted MRI in a patient with multiple sclerosis demonstrates
numerous white matter plaques in a callosal and pericallosal white
matter distribution. Axial
diffusion-weighted MRI in a patient with multiple sclerosis shows
several hyperintense lesions, a feature of inflammatory disease
activity. One of the limitations of using MRI in patients with
MS is the discordance occurring between lesion location and the
clinical presentation. In addition, depending on the number and location
of findings, MRI can vary greatly in terms of sensitivity and
specificity in the diagnosis of MS. This is especially true of primary
progressive MS, which may not show the classic discrete lesions of
relapsing-remitting MS.A clinician presented with an MRI report that details a few "nonspecific white matter lesions" that are "compatible with MS" is often frustrated with the lack of sensitivity and specificity of such a description. For this reason, imaging findings need to be described in detail, and preferably referenced to one of the published set of diagnostic criteria such as those by Paty[1] or Barkhof.[2] Finally, the specific patient's neurologic history and clinical findings must be correlated with the imaging to establish an accurate diagnosis.[3]
Plain radiographic studies have no positive predictive value in the diagnosis of multiple sclerosis, but occasionally, plain radiographs may be used to exclude mechanical bony lesions. Angiography also has a limited role in the diagnosis and management of MS, but when central nervous system (CNS) vasculitis is considered in a patient with undifferentiated findings, angiography may occasionally be considered.
Cerebrospinal fluid (CSF) analysis for oligoclonal banding or immunoglobulin G (IgG) levels is no longer routine in the investigation of MS, although this test may be of use when MRI is unavailable or MRI findings are nondiagnostic.[4]
Clinical diagnosis
A diagnosis of MS is made on the basis of clinical findings by using supporting evidence from ancillary tests such as CSF examination for oligoclonal banding and MRI.[5, 6, 7]Clinically, MS has historically been diagnosed via the demonstration of white matter dysfunction disseminated in time and space.[8] With the advent of diagnostic laboratory investigations and imaging techniques, the Poser criteria were proposed to establish a degree of certainty of diagnosis in the absence of the 2 clinical attacks by using terms such as possible MS and probable MS.[9]
With increasing treatment options for MS and better imaging techniques, newer diagnostic criteria have been suggested that allow diagnosis after a single attack coupled with appropriate positive test results. These criteria have been coined the MacDonald criteria.[10] Essentially, they allow for the second attack in time to be defined by a new lesion appearing on MRI. Also, the MacDonald criteria allow the dissemination in space to be established on the basis of either 9 typical white matter lesions on MRI or 1 enhancing lesion. If CSF studies show increased IgG values or oligoclonal banding, the presence of only 2 typical MRI lesions satisfy the dissemination-in-time criteria.
With respect to the initial clinical presentation in MS, it may vary with the white matter tract involved, and it may include somatic sensory changes, optic neuritis, or weakness, to mention just a few possible neurologic presentations. After only a single attack, the diagnosis of MS is suggested if the first impairment is coupled with positive paraclinical test results, such as those on imaging or CSF studies. Furthermore, the attack must be compatible with the pattern of impairment found in patients with MS, which typically means that the duration of deficit is days to weeks. Worsening of vision due to optic neuritis and subsequent exercise is known as the Uhthoff phenomenon.
Stankiewicz et al correlated brain lesions and clinical status with 1.5T and 3T MRI in 32 patients with MS by use of MRI fluid-attenuated inversion-recovery (FLAIR) sequences, and the authors found that MRI at 3T may provide increased sensitivity and validity in assessment of MS brain lesions. The study showed that FLAIR lesion volume (FLLV) at 3T was higher than at 1.5T. While 3T FLLV correlated moderately and significantly, 1.5T FLLV correlated poorly. When controlling for age and depression, correlations between FLLV and cognitive measures were significant at 1.5T for the Judgment of Line Orientation Test, the Symbol Digit Modalities Test, and the California Verbal Learning Test Delayed Free Recall, but at 3T, correlations were significant and of greater magnitude.[11]
Clinical course
The clinical course of MS can follow different patterns, and this observation has led to the classification of distinct types of MS. The most common form of MS is termed relapsing-remitting MS, in which progression involves symptoms of neurologic dysfunction frequently followed by partial or complete clinical recovery. In relapsing-remitting MS, global clinical deterioration has traditionally been attributed to cumulative deficit due to incomplete recovery from repeated occurrences of individual relapses. However, this cumulative deficit has been questioned, because evidence increasingly suggests an ongoing background neurologic deterioration that is independent of the relapses.Occasionally, the course of MS may be more indolent and exhibit a chronic, persistent neurologic deficit without apparent ongoing deterioration or further impairment. Sometimes, this course of MS is called inactive or benign MS, and this form is often observed in patients with prior relapsing-remitting disease.
Another potentially complicating matter clinically is that highly active MS lesions may sometimes demonstrate significant mass effect. Rarely, mass effect can lead to midline shift, herniations, infarctions, and even death. Such a drastic clinical and radiologic presentation can lead to an incorrect preliminary diagnosis and inappropriate neurosurgical intervention. When MS presents in a more fulminant, aggressive manner, it is frequently known as malignant MS or the Marburg variant.
In a prospective study, Lebrun et al followed 70 patients who had their first brain MRI for a variety of medical symptoms not suggestive of MS and found the mean time between the first brain MRI and the first clinically isolated syndrome to be 2.3 years (range, 0.8-5 y). Diagnostic studies of the blood, CSF, and visual evoked potentials were conducted, and clinical conversion occurred in 23 patients: 6 to optic neuritis, 6 to myelitis, 5 to brainstem symptoms, 4 to sensitive symptoms, 1 to cerebellar symptoms, and 1 to cognitive deterioration.[12] For patient education information, see Multiple Sclerosis.
No comments:
Post a Comment